Seung-Hun You, Sun-Young Jung, Hyun Joo Lee, Sulhee Kim, Eunjin Yang
{"title":"结合基于电子病历的实时自动警报系统可以改善快速反应系统:一项回顾性队列研究。","authors":"Seung-Hun You, Sun-Young Jung, Hyun Joo Lee, Sulhee Kim, Eunjin Yang","doi":"10.1186/s13049-021-00979-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rapid response systems (RRSs) are essential components of patient safety systems; however, limited evidence exists regarding their effectiveness and optimal structures. We aimed to assess the activation patterns and outcomes of RRS implementation with/without a real-time automatic alerting system (AAS) based on electronic medical records (EMRs).</p><p><strong>Methods: </strong>We retrospectively analyzed clinical data of patients for whom the RRS was activated in the surgical wards of a tertiary university hospital. We compared the code rate, in-hospital mortality, unplanned intensive care unit (ICU) admission, and other clinical outcomes before and after applying RRS and AAS as follows: pre-RRS (January 2013-July 2015), RRS without AAS (August 2015-November 2016), and RRS with AAS (December 2016-December 2017).</p><p><strong>Results: </strong>In-hospital mortality per 1000 admissions decreased from 15.1 to 12.9 after RRS implementation (p < 0.001). RRS activation per 1000 admissions increased from 14.4 to 26.3 after AAS implementation. The severity of patients' condition calculated using the modified early warning score increased from 2.5 (± 2.1) in the RRS without AAS to 3.6 (± 2.1) (p < 0.001) in the RRS with AAS. The total and preventable code rates and in-hospital mortality rates were comparable between the RRS implementation periods without/with AAS. ICU duration and mortality results improved in patients with RRS activation and unplanned ICU admission. The data of RRS non-activated group remained unaltered during the study.</p><p><strong>Conclusions: </strong>Real-time AAS based on EMRs might help identify unstable patients. Early detection and intervention with RRS may improve patient outcomes.</p>","PeriodicalId":501057,"journal":{"name":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","volume":" ","pages":"164"},"PeriodicalIF":0.0000,"publicationDate":"2021-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8643026/pdf/","citationCount":"3","resultStr":"{\"title\":\"Incorporating a real-time automatic alerting system based on electronic medical records could improve rapid response systems: a retrospective cohort study.\",\"authors\":\"Seung-Hun You, Sun-Young Jung, Hyun Joo Lee, Sulhee Kim, Eunjin Yang\",\"doi\":\"10.1186/s13049-021-00979-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Rapid response systems (RRSs) are essential components of patient safety systems; however, limited evidence exists regarding their effectiveness and optimal structures. We aimed to assess the activation patterns and outcomes of RRS implementation with/without a real-time automatic alerting system (AAS) based on electronic medical records (EMRs).</p><p><strong>Methods: </strong>We retrospectively analyzed clinical data of patients for whom the RRS was activated in the surgical wards of a tertiary university hospital. We compared the code rate, in-hospital mortality, unplanned intensive care unit (ICU) admission, and other clinical outcomes before and after applying RRS and AAS as follows: pre-RRS (January 2013-July 2015), RRS without AAS (August 2015-November 2016), and RRS with AAS (December 2016-December 2017).</p><p><strong>Results: </strong>In-hospital mortality per 1000 admissions decreased from 15.1 to 12.9 after RRS implementation (p < 0.001). RRS activation per 1000 admissions increased from 14.4 to 26.3 after AAS implementation. The severity of patients' condition calculated using the modified early warning score increased from 2.5 (± 2.1) in the RRS without AAS to 3.6 (± 2.1) (p < 0.001) in the RRS with AAS. The total and preventable code rates and in-hospital mortality rates were comparable between the RRS implementation periods without/with AAS. ICU duration and mortality results improved in patients with RRS activation and unplanned ICU admission. The data of RRS non-activated group remained unaltered during the study.</p><p><strong>Conclusions: </strong>Real-time AAS based on EMRs might help identify unstable patients. Early detection and intervention with RRS may improve patient outcomes.</p>\",\"PeriodicalId\":501057,\"journal\":{\"name\":\"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine\",\"volume\":\" \",\"pages\":\"164\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-12-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8643026/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13049-021-00979-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-021-00979-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Incorporating a real-time automatic alerting system based on electronic medical records could improve rapid response systems: a retrospective cohort study.
Background: Rapid response systems (RRSs) are essential components of patient safety systems; however, limited evidence exists regarding their effectiveness and optimal structures. We aimed to assess the activation patterns and outcomes of RRS implementation with/without a real-time automatic alerting system (AAS) based on electronic medical records (EMRs).
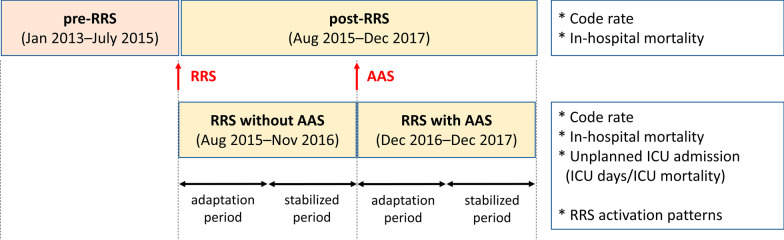
Methods: We retrospectively analyzed clinical data of patients for whom the RRS was activated in the surgical wards of a tertiary university hospital. We compared the code rate, in-hospital mortality, unplanned intensive care unit (ICU) admission, and other clinical outcomes before and after applying RRS and AAS as follows: pre-RRS (January 2013-July 2015), RRS without AAS (August 2015-November 2016), and RRS with AAS (December 2016-December 2017).
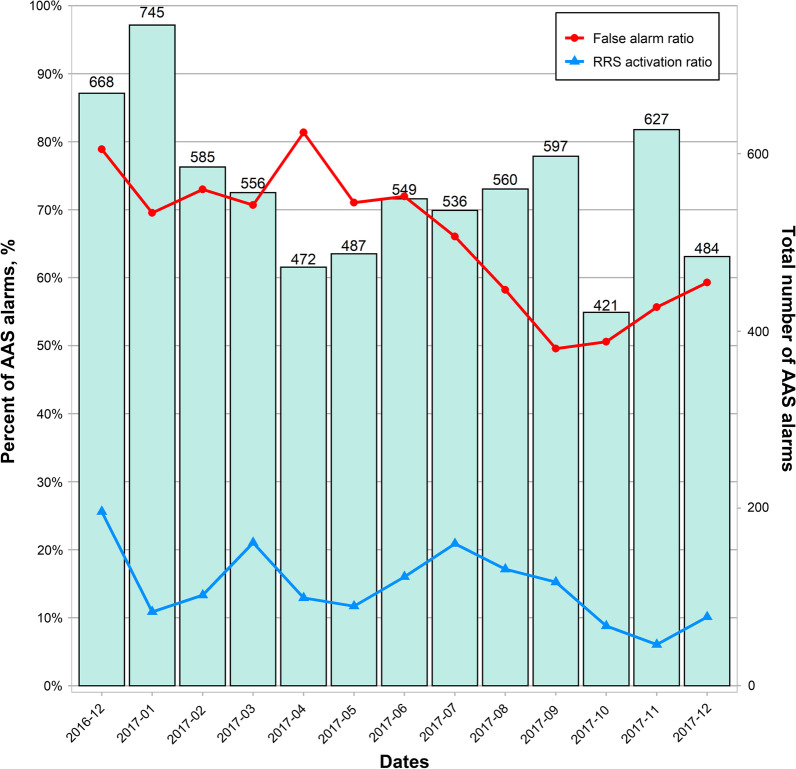
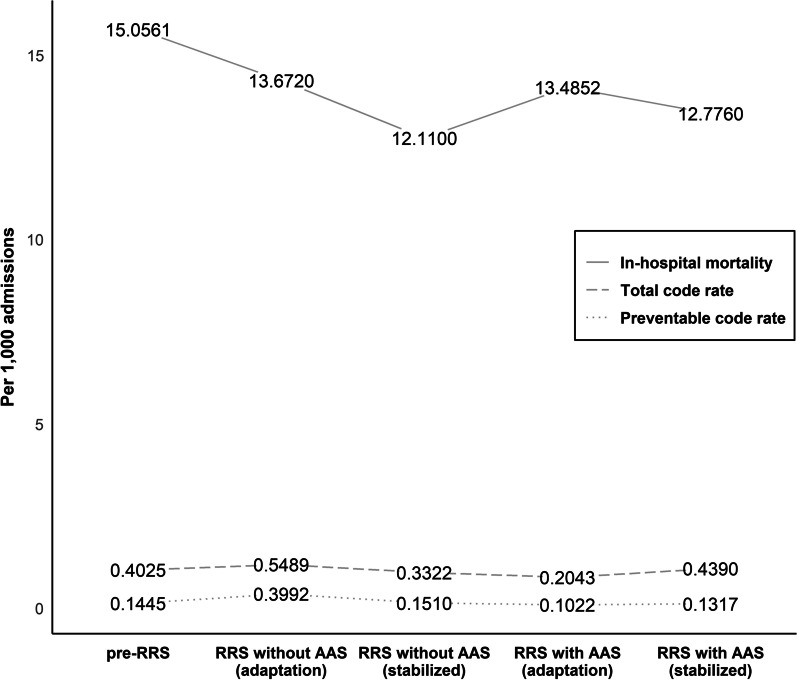
Results: In-hospital mortality per 1000 admissions decreased from 15.1 to 12.9 after RRS implementation (p < 0.001). RRS activation per 1000 admissions increased from 14.4 to 26.3 after AAS implementation. The severity of patients' condition calculated using the modified early warning score increased from 2.5 (± 2.1) in the RRS without AAS to 3.6 (± 2.1) (p < 0.001) in the RRS with AAS. The total and preventable code rates and in-hospital mortality rates were comparable between the RRS implementation periods without/with AAS. ICU duration and mortality results improved in patients with RRS activation and unplanned ICU admission. The data of RRS non-activated group remained unaltered during the study.
Conclusions: Real-time AAS based on EMRs might help identify unstable patients. Early detection and intervention with RRS may improve patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


