Boel De Paepe , Ken R. Bracke , Jan L. De Bleecker
{"title":"一项关于肌肉疾病患者循环细胞因子和趋化因子的探索性研究表明,CD40L和CCL5是一般疾病标志物,而CXCL10是自身免疫性肌炎患者的鉴别标志物","authors":"Boel De Paepe , Ken R. Bracke , Jan L. De Bleecker","doi":"10.1016/j.cytox.2022.100063","DOIUrl":null,"url":null,"abstract":"<div><p>Discriminating an autoimmune myositis from other disorders and subtyping of patient groups within this heterogeneous group of conditions remain diagnostic challenges. In our study we explored the potential of cytokine and chemokine typing in patient sera as an addition to the expanding set of blood-accessible diagnostic biomarkers available today. We selected sets of ten patients within well-characterized disease groups representing healthy controls, and patients with hereditary muscular dystrophies, immune-mediated necrotizing myopathy (IMNM) and sporadic inclusion body myositis (IBM). Prescreening using proteome arrays singled out three biomarker candidates, being the cytokine CD40L, and chemokines CXCL10 and CCL5. Enzyme-linked immunosorbent assays showed all three markers to be elevated in muscle disease irrespective of patient subgroup. CXCL10 levels on the other hand were higher in autoimmune myositis only, and levels were significantly higher in IBM compared to IMNM. The strong CXCL10 expression observed in the auto-aggressive inflammatory cells within IBM muscle tissues possibly represents a major source of circulating CXCL10. We conclude that CXCL10 levels could represent a convenient marker for autoimmune myositis indicative of patient subgroups.</p></div>","PeriodicalId":37028,"journal":{"name":"Cytokine: X","volume":"4 1","pages":"Article 100063"},"PeriodicalIF":0.0000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/15/b0/main.PMC8803590.pdf","citationCount":"3","resultStr":"{\"title\":\"An exploratory study of circulating cytokines and chemokines in patients with muscle disorders proposes CD40L and CCL5 represent general disease markers while CXCL10 differentiates between patients with an autoimmune myositis\",\"authors\":\"Boel De Paepe , Ken R. Bracke , Jan L. De Bleecker\",\"doi\":\"10.1016/j.cytox.2022.100063\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>Discriminating an autoimmune myositis from other disorders and subtyping of patient groups within this heterogeneous group of conditions remain diagnostic challenges. In our study we explored the potential of cytokine and chemokine typing in patient sera as an addition to the expanding set of blood-accessible diagnostic biomarkers available today. We selected sets of ten patients within well-characterized disease groups representing healthy controls, and patients with hereditary muscular dystrophies, immune-mediated necrotizing myopathy (IMNM) and sporadic inclusion body myositis (IBM). Prescreening using proteome arrays singled out three biomarker candidates, being the cytokine CD40L, and chemokines CXCL10 and CCL5. Enzyme-linked immunosorbent assays showed all three markers to be elevated in muscle disease irrespective of patient subgroup. CXCL10 levels on the other hand were higher in autoimmune myositis only, and levels were significantly higher in IBM compared to IMNM. The strong CXCL10 expression observed in the auto-aggressive inflammatory cells within IBM muscle tissues possibly represents a major source of circulating CXCL10. We conclude that CXCL10 levels could represent a convenient marker for autoimmune myositis indicative of patient subgroups.</p></div>\",\"PeriodicalId\":37028,\"journal\":{\"name\":\"Cytokine: X\",\"volume\":\"4 1\",\"pages\":\"Article 100063\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/15/b0/main.PMC8803590.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cytokine: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590153222000027\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cytokine: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590153222000027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
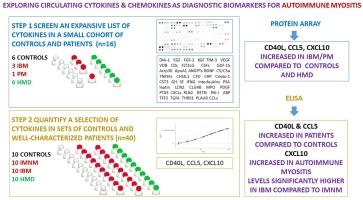
An exploratory study of circulating cytokines and chemokines in patients with muscle disorders proposes CD40L and CCL5 represent general disease markers while CXCL10 differentiates between patients with an autoimmune myositis
Discriminating an autoimmune myositis from other disorders and subtyping of patient groups within this heterogeneous group of conditions remain diagnostic challenges. In our study we explored the potential of cytokine and chemokine typing in patient sera as an addition to the expanding set of blood-accessible diagnostic biomarkers available today. We selected sets of ten patients within well-characterized disease groups representing healthy controls, and patients with hereditary muscular dystrophies, immune-mediated necrotizing myopathy (IMNM) and sporadic inclusion body myositis (IBM). Prescreening using proteome arrays singled out three biomarker candidates, being the cytokine CD40L, and chemokines CXCL10 and CCL5. Enzyme-linked immunosorbent assays showed all three markers to be elevated in muscle disease irrespective of patient subgroup. CXCL10 levels on the other hand were higher in autoimmune myositis only, and levels were significantly higher in IBM compared to IMNM. The strong CXCL10 expression observed in the auto-aggressive inflammatory cells within IBM muscle tissues possibly represents a major source of circulating CXCL10. We conclude that CXCL10 levels could represent a convenient marker for autoimmune myositis indicative of patient subgroups.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


