Anadeijda J E M C Landman, Marjon A de Boer, Laura Visser, Tobias A J Nijman, Marieke A C Hemels, Christiana N Naaktgeboren, Marijke C van der Weide, Ben W Mol, Judith O E H van Laar, Dimitri N M Papatsonis, Mireille N Bekker, Joris van Drongelen, Mariëlle G van Pampus, Marieke Sueters, David P van der Ham, J Marko Sikkema, Joost J Zwart, Anjoke J M Huisjes, Marloes E van Huizen, Gunilla Kleiverda, Janine Boon, Maureen T M Franssen, Wietske Hermes, Harry Visser, Christianne J M de Groot, Martijn A Oudijk
{"title":"低剂量阿司匹林预防复发性自发性早产的评价(APRIL研究):一项多中心、随机、双盲、安慰剂对照试验。","authors":"Anadeijda J E M C Landman, Marjon A de Boer, Laura Visser, Tobias A J Nijman, Marieke A C Hemels, Christiana N Naaktgeboren, Marijke C van der Weide, Ben W Mol, Judith O E H van Laar, Dimitri N M Papatsonis, Mireille N Bekker, Joris van Drongelen, Mariëlle G van Pampus, Marieke Sueters, David P van der Ham, J Marko Sikkema, Joost J Zwart, Anjoke J M Huisjes, Marloes E van Huizen, Gunilla Kleiverda, Janine Boon, Maureen T M Franssen, Wietske Hermes, Harry Visser, Christianne J M de Groot, Martijn A Oudijk","doi":"10.1371/journal.pmed.1003892","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Preterm birth is the leading cause of neonatal morbidity and mortality. The recurrence rate of spontaneous preterm birth is high, and additional preventive measures are required. Our objective was to assess the effectiveness of low-dose aspirin compared to placebo in the prevention of preterm birth in women with a previous spontaneous preterm birth.</p><p><strong>Methods and findings: </strong>We performed a parallel multicentre, randomised, double-blinded, placebo-controlled trial (the APRIL study). The study was performed in 8 tertiary and 26 secondary care hospitals in the Netherlands. We included women with a singleton pregnancy and a history of spontaneous preterm birth of a singleton between 22 and 37 weeks. Participants were randomly assigned to aspirin 80 mg daily or placebo initiated between 8 and 16 weeks of gestation and continued until 36 weeks or delivery. Randomisation was computer generated, with allocation concealment by using sequentially numbered medication containers. Participants, their healthcare providers, and researchers were blinded for treatment allocation. The primary outcome was preterm birth <37 weeks of gestation. Secondary outcomes included a composite of poor neonatal outcome (bronchopulmonary dysplasia, periventricular leukomalacia > grade 1, intraventricular hemorrhage > grade 2, necrotising enterocolitis > stage 1, retinopathy of prematurity, culture proven sepsis, or perinatal death). Analyses were performed by intention to treat. From May 31, 2016 to June 13, 2019, 406 women were randomised to aspirin (n = 204) or placebo (n = 202). A total of 387 women (81.1% of white ethnic origin, mean age 32.5 ± SD 3.8) were included in the final analysis: 194 women were allocated to aspirin and 193 to placebo. Preterm birth <37 weeks occurred in 41 (21.2%) women in the aspirin group and 49 (25.4%) in the placebo group (relative risk (RR) 0.83, 95% confidence interval (CI) 0.58 to 1.20, p = 0.32). In women with ≥80% medication adherence, preterm birth occurred in 24 (19.2%) versus 30 (24.8%) women (RR 0.77, 95% CI 0.48 to 1.25, p = 0.29). The rate of the composite of poor neonatal outcome was 4.6% (n = 9) versus 2.6% (n = 5) (RR 1.79, 95% CI 0.61 to 5.25, p = 0.29). Among all randomised women, serious adverse events occurred in 11 out of 204 (5.4%) women allocated to aspirin and 11 out of 202 (5.4%) women allocated to placebo. None of these serious adverse events was considered to be associated with treatment allocation. The main study limitation is the underpowered sample size due to the lower than expected preterm birth rates.</p><p><strong>Conclusions: </strong>In this study, we observed that low-dose aspirin did not significantly reduce the preterm birth rate in women with a previous spontaneous preterm birth. However, a modest reduction of preterm birth with aspirin cannot be ruled out. Further research is required to determine a possible beneficial effect of low-dose aspirin for women with a previous spontaneous preterm birth.</p><p><strong>Trial registration: </strong>Dutch Trial Register (NL5553, NTR5675) https://www.trialregister.nl/trial/5553.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 2","pages":"e1003892"},"PeriodicalIF":9.9000,"publicationDate":"2022-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8806064/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of low-dose aspirin in the prevention of recurrent spontaneous preterm labour (the APRIL study): A multicentre, randomised, double-blinded, placebo-controlled trial.\",\"authors\":\"Anadeijda J E M C Landman, Marjon A de Boer, Laura Visser, Tobias A J Nijman, Marieke A C Hemels, Christiana N Naaktgeboren, Marijke C van der Weide, Ben W Mol, Judith O E H van Laar, Dimitri N M Papatsonis, Mireille N Bekker, Joris van Drongelen, Mariëlle G van Pampus, Marieke Sueters, David P van der Ham, J Marko Sikkema, Joost J Zwart, Anjoke J M Huisjes, Marloes E van Huizen, Gunilla Kleiverda, Janine Boon, Maureen T M Franssen, Wietske Hermes, Harry Visser, Christianne J M de Groot, Martijn A Oudijk\",\"doi\":\"10.1371/journal.pmed.1003892\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Preterm birth is the leading cause of neonatal morbidity and mortality. The recurrence rate of spontaneous preterm birth is high, and additional preventive measures are required. Our objective was to assess the effectiveness of low-dose aspirin compared to placebo in the prevention of preterm birth in women with a previous spontaneous preterm birth.</p><p><strong>Methods and findings: </strong>We performed a parallel multicentre, randomised, double-blinded, placebo-controlled trial (the APRIL study). The study was performed in 8 tertiary and 26 secondary care hospitals in the Netherlands. We included women with a singleton pregnancy and a history of spontaneous preterm birth of a singleton between 22 and 37 weeks. Participants were randomly assigned to aspirin 80 mg daily or placebo initiated between 8 and 16 weeks of gestation and continued until 36 weeks or delivery. Randomisation was computer generated, with allocation concealment by using sequentially numbered medication containers. Participants, their healthcare providers, and researchers were blinded for treatment allocation. The primary outcome was preterm birth <37 weeks of gestation. Secondary outcomes included a composite of poor neonatal outcome (bronchopulmonary dysplasia, periventricular leukomalacia > grade 1, intraventricular hemorrhage > grade 2, necrotising enterocolitis > stage 1, retinopathy of prematurity, culture proven sepsis, or perinatal death). Analyses were performed by intention to treat. From May 31, 2016 to June 13, 2019, 406 women were randomised to aspirin (n = 204) or placebo (n = 202). A total of 387 women (81.1% of white ethnic origin, mean age 32.5 ± SD 3.8) were included in the final analysis: 194 women were allocated to aspirin and 193 to placebo. Preterm birth <37 weeks occurred in 41 (21.2%) women in the aspirin group and 49 (25.4%) in the placebo group (relative risk (RR) 0.83, 95% confidence interval (CI) 0.58 to 1.20, p = 0.32). In women with ≥80% medication adherence, preterm birth occurred in 24 (19.2%) versus 30 (24.8%) women (RR 0.77, 95% CI 0.48 to 1.25, p = 0.29). The rate of the composite of poor neonatal outcome was 4.6% (n = 9) versus 2.6% (n = 5) (RR 1.79, 95% CI 0.61 to 5.25, p = 0.29). Among all randomised women, serious adverse events occurred in 11 out of 204 (5.4%) women allocated to aspirin and 11 out of 202 (5.4%) women allocated to placebo. None of these serious adverse events was considered to be associated with treatment allocation. The main study limitation is the underpowered sample size due to the lower than expected preterm birth rates.</p><p><strong>Conclusions: </strong>In this study, we observed that low-dose aspirin did not significantly reduce the preterm birth rate in women with a previous spontaneous preterm birth. However, a modest reduction of preterm birth with aspirin cannot be ruled out. Further research is required to determine a possible beneficial effect of low-dose aspirin for women with a previous spontaneous preterm birth.</p><p><strong>Trial registration: </strong>Dutch Trial Register (NL5553, NTR5675) https://www.trialregister.nl/trial/5553.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 2\",\"pages\":\"e1003892\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2022-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8806064/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003892\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003892","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Evaluation of low-dose aspirin in the prevention of recurrent spontaneous preterm labour (the APRIL study): A multicentre, randomised, double-blinded, placebo-controlled trial.
Background: Preterm birth is the leading cause of neonatal morbidity and mortality. The recurrence rate of spontaneous preterm birth is high, and additional preventive measures are required. Our objective was to assess the effectiveness of low-dose aspirin compared to placebo in the prevention of preterm birth in women with a previous spontaneous preterm birth.
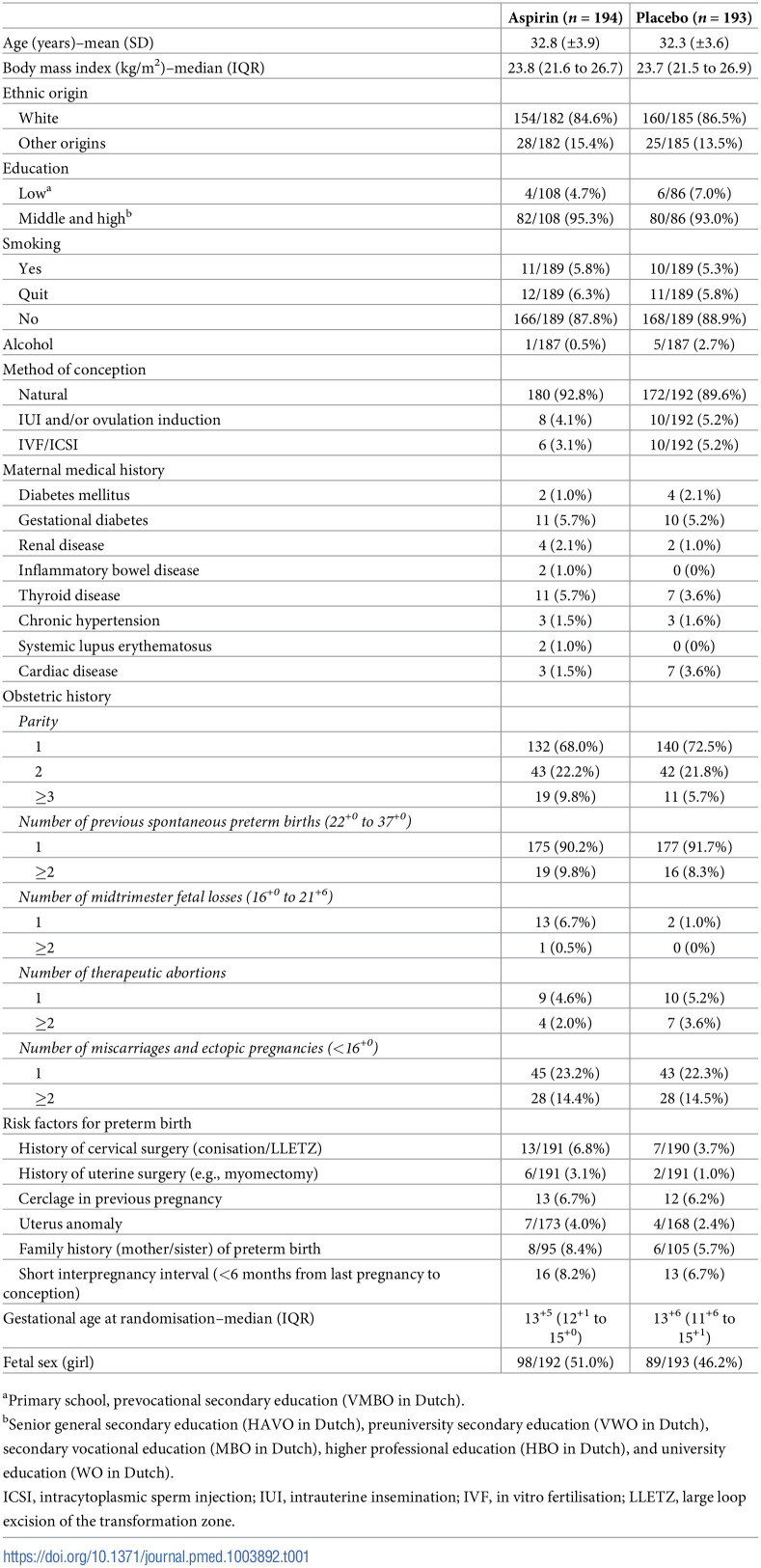
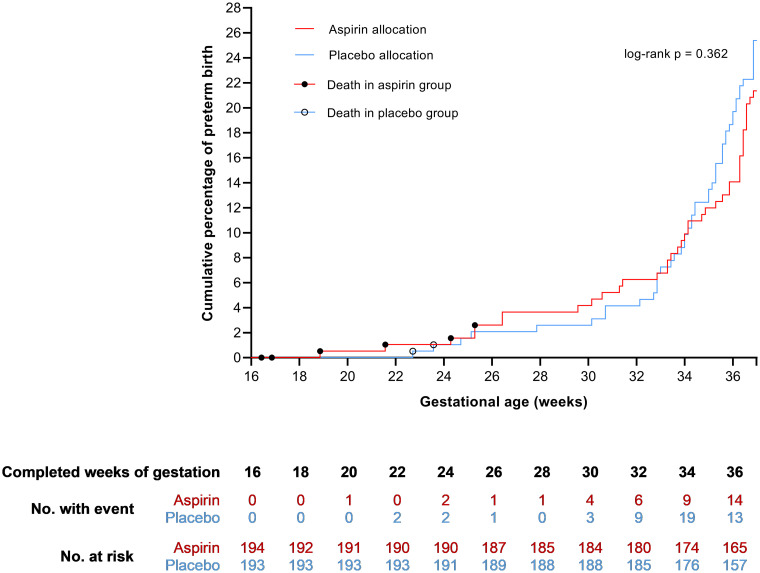
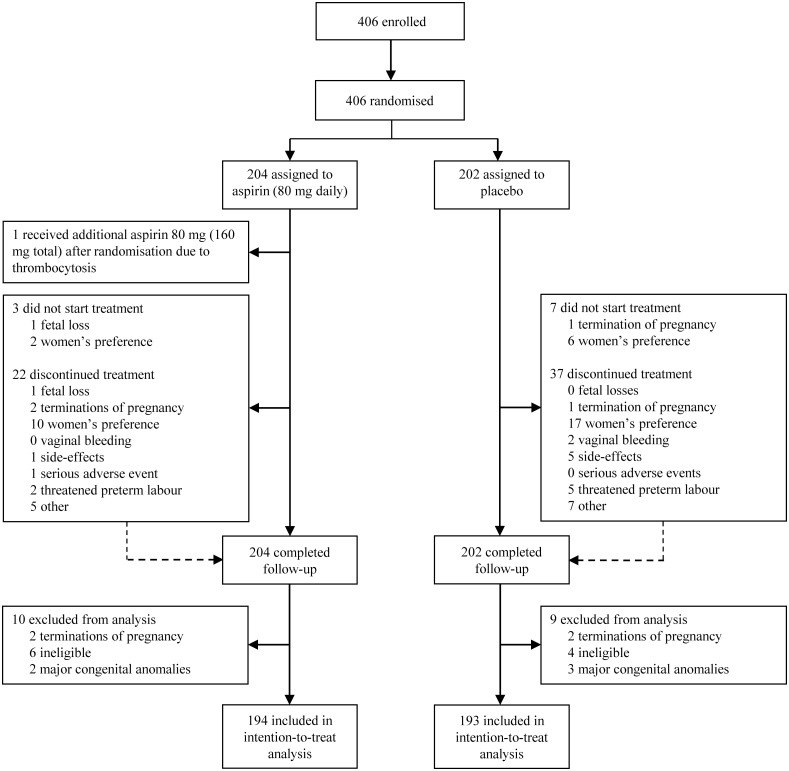
Methods and findings: We performed a parallel multicentre, randomised, double-blinded, placebo-controlled trial (the APRIL study). The study was performed in 8 tertiary and 26 secondary care hospitals in the Netherlands. We included women with a singleton pregnancy and a history of spontaneous preterm birth of a singleton between 22 and 37 weeks. Participants were randomly assigned to aspirin 80 mg daily or placebo initiated between 8 and 16 weeks of gestation and continued until 36 weeks or delivery. Randomisation was computer generated, with allocation concealment by using sequentially numbered medication containers. Participants, their healthcare providers, and researchers were blinded for treatment allocation. The primary outcome was preterm birth <37 weeks of gestation. Secondary outcomes included a composite of poor neonatal outcome (bronchopulmonary dysplasia, periventricular leukomalacia > grade 1, intraventricular hemorrhage > grade 2, necrotising enterocolitis > stage 1, retinopathy of prematurity, culture proven sepsis, or perinatal death). Analyses were performed by intention to treat. From May 31, 2016 to June 13, 2019, 406 women were randomised to aspirin (n = 204) or placebo (n = 202). A total of 387 women (81.1% of white ethnic origin, mean age 32.5 ± SD 3.8) were included in the final analysis: 194 women were allocated to aspirin and 193 to placebo. Preterm birth <37 weeks occurred in 41 (21.2%) women in the aspirin group and 49 (25.4%) in the placebo group (relative risk (RR) 0.83, 95% confidence interval (CI) 0.58 to 1.20, p = 0.32). In women with ≥80% medication adherence, preterm birth occurred in 24 (19.2%) versus 30 (24.8%) women (RR 0.77, 95% CI 0.48 to 1.25, p = 0.29). The rate of the composite of poor neonatal outcome was 4.6% (n = 9) versus 2.6% (n = 5) (RR 1.79, 95% CI 0.61 to 5.25, p = 0.29). Among all randomised women, serious adverse events occurred in 11 out of 204 (5.4%) women allocated to aspirin and 11 out of 202 (5.4%) women allocated to placebo. None of these serious adverse events was considered to be associated with treatment allocation. The main study limitation is the underpowered sample size due to the lower than expected preterm birth rates.
Conclusions: In this study, we observed that low-dose aspirin did not significantly reduce the preterm birth rate in women with a previous spontaneous preterm birth. However, a modest reduction of preterm birth with aspirin cannot be ruled out. Further research is required to determine a possible beneficial effect of low-dose aspirin for women with a previous spontaneous preterm birth.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


