Gregory A Nuttall, Mark M Smith, Bradford B Smith, Jon M Christensen, Paula J Santrach, Hartzell V Schaff
{"title":"一项比较体外循环心脏手术患者标准活化凝血时间肝素管理与高目标活化凝血时间和个体化Hepcon HMS肝素管理的随机盲法试验。","authors":"Gregory A Nuttall, Mark M Smith, Bradford B Smith, Jon M Christensen, Paula J Santrach, Hartzell V Schaff","doi":"10.5761/atcs.oa.21-00222","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>High-dose heparin has been suggested to reduce consumption coagulopathy.</p><p><strong>Materials and methods: </strong>In a randomized, blinded, prospective trial of patients undergoing elective, complex cardiac surgery with cardiopulmonary bypass, patients were randomized to one of three groups: 1) high-dose heparin (HH) receiving an initial heparin dose of 450 u/kg, 2) heparin concentration monitoring (HC) with Hepcon Hemostasis Management System (HMS; Medtronic, Minneapolis, MN, USA) monitoring, or 3) a control group (C) receiving a standard heparin dose of 300 u/kg. Primary outcome measures were blood loss and transfusion requirements.</p><p><strong>Results: </strong>There were 269 patients block randomized based on primary versus redo sternotomy to one of the three groups from August 2001 to August 2003. There was no difference in operative bleeding between the groups. Chest tube drainage did not differ between treatment groups at 8 hours (median [25th percentile, 75th percentile] for control group was 321 [211, 490] compared to 340 [210, 443] and 327 [250, 545], p = 0.998 and p = 0.540, for HH and HC treatment groups, respectively). The percentage of patients receiving transfusion was not different among the groups.</p><p><strong>Conclusion: </strong>Higher heparin dosing accomplished by either activated clot time or HC monitoring did not reduce 24-hour intensive care unit blood loss or transfusion requirements.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"28 3","pages":"204-213"},"PeriodicalIF":1.3000,"publicationDate":"2022-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6b/6f/atcs-28-204.PMC9209891.pdf","citationCount":"2","resultStr":"{\"title\":\"A Blinded Randomized Trial Comparing Standard Activated Clotting Time Heparin Management to High Target Active Clotting Time and Individualized Hepcon HMS Heparin Management in Cardiopulmonary Bypass Cardiac Surgical Patients.\",\"authors\":\"Gregory A Nuttall, Mark M Smith, Bradford B Smith, Jon M Christensen, Paula J Santrach, Hartzell V Schaff\",\"doi\":\"10.5761/atcs.oa.21-00222\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>High-dose heparin has been suggested to reduce consumption coagulopathy.</p><p><strong>Materials and methods: </strong>In a randomized, blinded, prospective trial of patients undergoing elective, complex cardiac surgery with cardiopulmonary bypass, patients were randomized to one of three groups: 1) high-dose heparin (HH) receiving an initial heparin dose of 450 u/kg, 2) heparin concentration monitoring (HC) with Hepcon Hemostasis Management System (HMS; Medtronic, Minneapolis, MN, USA) monitoring, or 3) a control group (C) receiving a standard heparin dose of 300 u/kg. Primary outcome measures were blood loss and transfusion requirements.</p><p><strong>Results: </strong>There were 269 patients block randomized based on primary versus redo sternotomy to one of the three groups from August 2001 to August 2003. There was no difference in operative bleeding between the groups. Chest tube drainage did not differ between treatment groups at 8 hours (median [25th percentile, 75th percentile] for control group was 321 [211, 490] compared to 340 [210, 443] and 327 [250, 545], p = 0.998 and p = 0.540, for HH and HC treatment groups, respectively). The percentage of patients receiving transfusion was not different among the groups.</p><p><strong>Conclusion: </strong>Higher heparin dosing accomplished by either activated clot time or HC monitoring did not reduce 24-hour intensive care unit blood loss or transfusion requirements.</p>\",\"PeriodicalId\":8037,\"journal\":{\"name\":\"Annals of Thoracic and Cardiovascular Surgery\",\"volume\":\"28 3\",\"pages\":\"204-213\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6b/6f/atcs-28-204.PMC9209891.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.oa.21-00222\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/12/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.21-00222","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/22 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A Blinded Randomized Trial Comparing Standard Activated Clotting Time Heparin Management to High Target Active Clotting Time and Individualized Hepcon HMS Heparin Management in Cardiopulmonary Bypass Cardiac Surgical Patients.
Purpose: High-dose heparin has been suggested to reduce consumption coagulopathy.
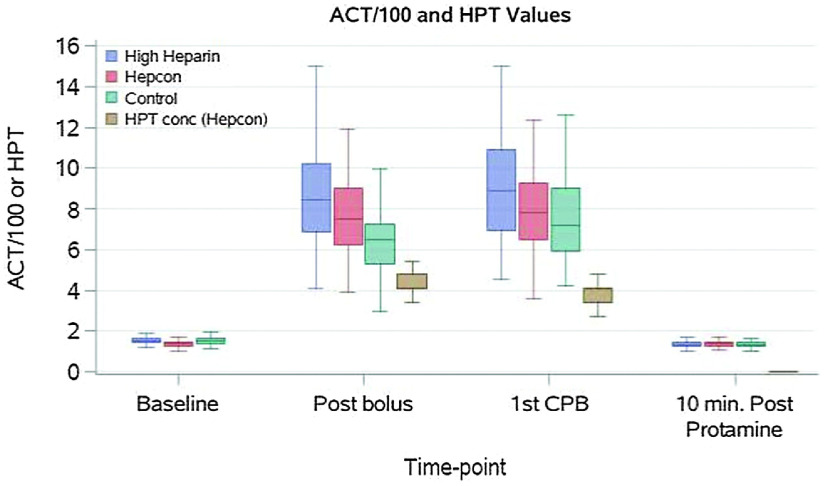
Materials and methods: In a randomized, blinded, prospective trial of patients undergoing elective, complex cardiac surgery with cardiopulmonary bypass, patients were randomized to one of three groups: 1) high-dose heparin (HH) receiving an initial heparin dose of 450 u/kg, 2) heparin concentration monitoring (HC) with Hepcon Hemostasis Management System (HMS; Medtronic, Minneapolis, MN, USA) monitoring, or 3) a control group (C) receiving a standard heparin dose of 300 u/kg. Primary outcome measures were blood loss and transfusion requirements.
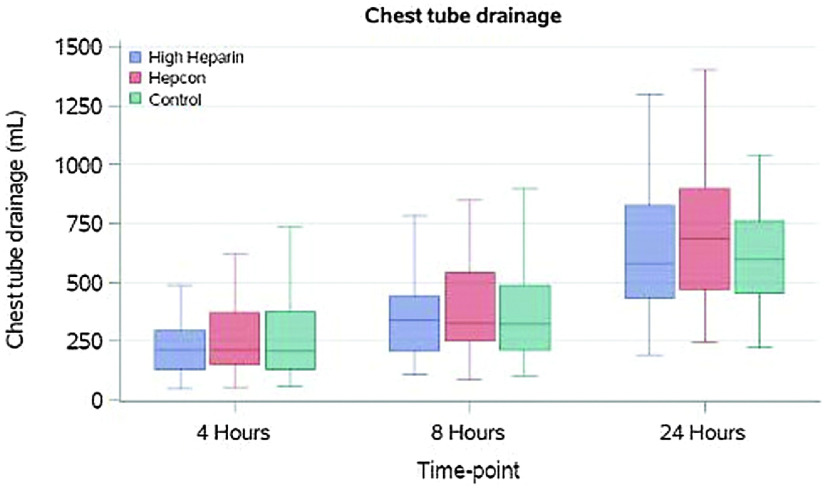
Results: There were 269 patients block randomized based on primary versus redo sternotomy to one of the three groups from August 2001 to August 2003. There was no difference in operative bleeding between the groups. Chest tube drainage did not differ between treatment groups at 8 hours (median [25th percentile, 75th percentile] for control group was 321 [211, 490] compared to 340 [210, 443] and 327 [250, 545], p = 0.998 and p = 0.540, for HH and HC treatment groups, respectively). The percentage of patients receiving transfusion was not different among the groups.
Conclusion: Higher heparin dosing accomplished by either activated clot time or HC monitoring did not reduce 24-hour intensive care unit blood loss or transfusion requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


