Valerie M Vaughn, Tejal N Gandhi, Timothy P Hofer, Lindsay A Petty, Anurag N Malani, Danielle Osterholzer, Lisa E Dumkow, David Ratz, Jennifer K Horowitz, Elizabeth S McLaughlin, Tawny Czilok, Scott A Flanders
{"title":"改善无并发症社区获得性肺炎住院患者抗生素持续时间和预后的全州协作质量倡议。","authors":"Valerie M Vaughn, Tejal N Gandhi, Timothy P Hofer, Lindsay A Petty, Anurag N Malani, Danielle Osterholzer, Lisa E Dumkow, David Ratz, Jennifer K Horowitz, Elizabeth S McLaughlin, Tawny Czilok, Scott A Flanders","doi":"10.1093/cid/ciab950","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Community-acquired pneumonia (CAP) is a common cause for hospitalization and antibiotic overuse. We aimed to improve antibiotic duration for CAP across 41 hospitals participating in the Michigan Hospital Medicine Safety Consortium (HMS).</p><p><strong>Methods: </strong>This prospective collaborative quality initiative included patients hospitalized with uncomplicated CAP who qualified for a 5-day antibiotic duration. Between 23 February 2017 and 5 February 2020, HMS targeted appropriate 5-day antibiotic treatment through benchmarking, sharing best practices, and pay-for-performance incentives. Changes in outcomes, including appropriate receipt of 5 ± 1-day antibiotic treatment and 30-day postdischarge composite adverse events (ie, deaths, readmissions, urgent visits, and antibiotic-associated adverse events), were assessed over time (per 3-month quarter), using logistic regression and controlling for hospital clustering.</p><p><strong>Results: </strong>A total of 41 hospitals and 6553 patients were included. The percentage of patients treated with an appropriate 5 ± 1-day duration increased from 22.1% (predicted probability, 20.9% [95% confidence interval: 17.2%-25.0%]) to 45.9% (predicted probability, 43.9% [36.8%-51.2%]; adjusted odds ratio [aOR] per quarter, 1.10 [1.07-1.14]). Thirty-day composite adverse events occurred in 18.5% of patients (1166 of 6319) and decreased over time (aOR per quarter, 0.98 [95% confidence interval: .96-.99]) owing to a decrease in antibiotic-associated adverse events (aOR per quarter, 0.91 [.87-.95]).</p><p><strong>Conclusions: </strong>Across diverse hospitals, HMS participation was associated with more appropriate use of short-course therapy and fewer adverse events in hospitalized patients with uncomplicated CAP. Establishment of national or regional collaborative quality initiatives with data collection and benchmarking, sharing of best practices, and pay-for-performance incentives may improve antibiotic use and outcomes for patients hospitalized with uncomplicated CAP.</p>","PeriodicalId":10421,"journal":{"name":"Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America","volume":" ","pages":"460-467"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/d0/ciab950.PMC9427146.pdf","citationCount":"4","resultStr":"{\"title\":\"A Statewide Collaborative Quality Initiative to Improve Antibiotic Duration and Outcomes in Patients Hospitalized With Uncomplicated Community-Acquired Pneumonia.\",\"authors\":\"Valerie M Vaughn, Tejal N Gandhi, Timothy P Hofer, Lindsay A Petty, Anurag N Malani, Danielle Osterholzer, Lisa E Dumkow, David Ratz, Jennifer K Horowitz, Elizabeth S McLaughlin, Tawny Czilok, Scott A Flanders\",\"doi\":\"10.1093/cid/ciab950\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Community-acquired pneumonia (CAP) is a common cause for hospitalization and antibiotic overuse. We aimed to improve antibiotic duration for CAP across 41 hospitals participating in the Michigan Hospital Medicine Safety Consortium (HMS).</p><p><strong>Methods: </strong>This prospective collaborative quality initiative included patients hospitalized with uncomplicated CAP who qualified for a 5-day antibiotic duration. Between 23 February 2017 and 5 February 2020, HMS targeted appropriate 5-day antibiotic treatment through benchmarking, sharing best practices, and pay-for-performance incentives. Changes in outcomes, including appropriate receipt of 5 ± 1-day antibiotic treatment and 30-day postdischarge composite adverse events (ie, deaths, readmissions, urgent visits, and antibiotic-associated adverse events), were assessed over time (per 3-month quarter), using logistic regression and controlling for hospital clustering.</p><p><strong>Results: </strong>A total of 41 hospitals and 6553 patients were included. The percentage of patients treated with an appropriate 5 ± 1-day duration increased from 22.1% (predicted probability, 20.9% [95% confidence interval: 17.2%-25.0%]) to 45.9% (predicted probability, 43.9% [36.8%-51.2%]; adjusted odds ratio [aOR] per quarter, 1.10 [1.07-1.14]). Thirty-day composite adverse events occurred in 18.5% of patients (1166 of 6319) and decreased over time (aOR per quarter, 0.98 [95% confidence interval: .96-.99]) owing to a decrease in antibiotic-associated adverse events (aOR per quarter, 0.91 [.87-.95]).</p><p><strong>Conclusions: </strong>Across diverse hospitals, HMS participation was associated with more appropriate use of short-course therapy and fewer adverse events in hospitalized patients with uncomplicated CAP. Establishment of national or regional collaborative quality initiatives with data collection and benchmarking, sharing of best practices, and pay-for-performance incentives may improve antibiotic use and outcomes for patients hospitalized with uncomplicated CAP.</p>\",\"PeriodicalId\":10421,\"journal\":{\"name\":\"Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America\",\"volume\":\" \",\"pages\":\"460-467\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f1/d0/ciab950.PMC9427146.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/cid/ciab950\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/cid/ciab950","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A Statewide Collaborative Quality Initiative to Improve Antibiotic Duration and Outcomes in Patients Hospitalized With Uncomplicated Community-Acquired Pneumonia.
Background: Community-acquired pneumonia (CAP) is a common cause for hospitalization and antibiotic overuse. We aimed to improve antibiotic duration for CAP across 41 hospitals participating in the Michigan Hospital Medicine Safety Consortium (HMS).
Methods: This prospective collaborative quality initiative included patients hospitalized with uncomplicated CAP who qualified for a 5-day antibiotic duration. Between 23 February 2017 and 5 February 2020, HMS targeted appropriate 5-day antibiotic treatment through benchmarking, sharing best practices, and pay-for-performance incentives. Changes in outcomes, including appropriate receipt of 5 ± 1-day antibiotic treatment and 30-day postdischarge composite adverse events (ie, deaths, readmissions, urgent visits, and antibiotic-associated adverse events), were assessed over time (per 3-month quarter), using logistic regression and controlling for hospital clustering.
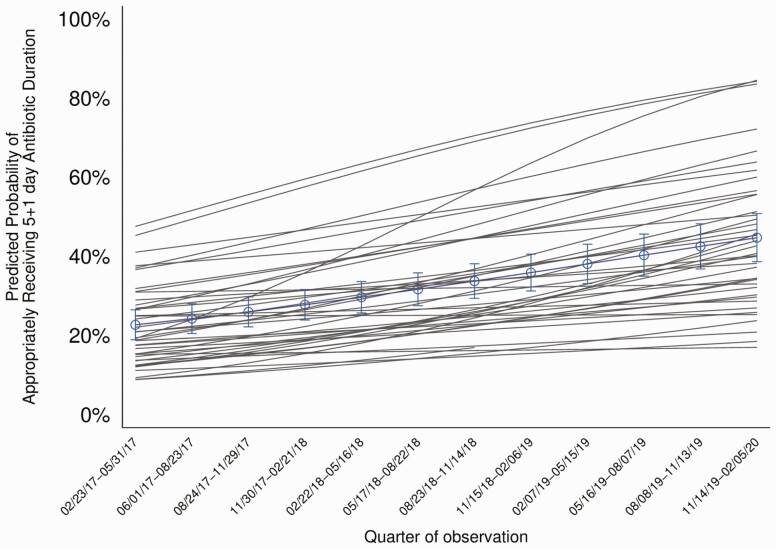
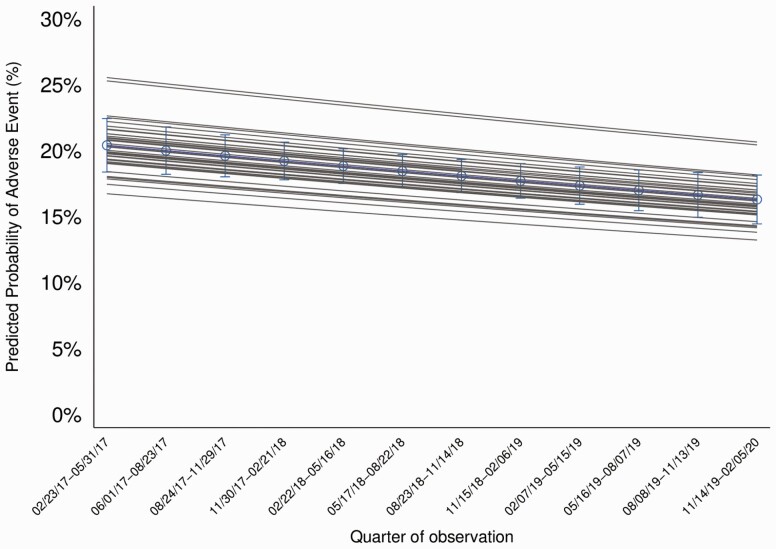
Results: A total of 41 hospitals and 6553 patients were included. The percentage of patients treated with an appropriate 5 ± 1-day duration increased from 22.1% (predicted probability, 20.9% [95% confidence interval: 17.2%-25.0%]) to 45.9% (predicted probability, 43.9% [36.8%-51.2%]; adjusted odds ratio [aOR] per quarter, 1.10 [1.07-1.14]). Thirty-day composite adverse events occurred in 18.5% of patients (1166 of 6319) and decreased over time (aOR per quarter, 0.98 [95% confidence interval: .96-.99]) owing to a decrease in antibiotic-associated adverse events (aOR per quarter, 0.91 [.87-.95]).
Conclusions: Across diverse hospitals, HMS participation was associated with more appropriate use of short-course therapy and fewer adverse events in hospitalized patients with uncomplicated CAP. Establishment of national or regional collaborative quality initiatives with data collection and benchmarking, sharing of best practices, and pay-for-performance incentives may improve antibiotic use and outcomes for patients hospitalized with uncomplicated CAP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


