Arezou Zoroufian, Ali Vasheghani-Farahani, Neda Toofaninejad
{"title":"房间隔缺损导致左心室起搏导联错位。","authors":"Arezou Zoroufian, Ali Vasheghani-Farahani, Neda Toofaninejad","doi":"10.18502/jthc.v16i2.7393","DOIUrl":null,"url":null,"abstract":"<p><p>A 54-year-old woman with a history of unknown childhood cardiac surgery underwent dual-chamber pacemaker implantation due to an advanced atrioventricular block in our center. One week later, we were asked to further evaluate tricuspid regurgitation via transthoracic echocardiography (TTE). The postoperative TTE demonstrated a left ventricular ejection fraction of 45%, as well as moderate mitral regurgitation, a severely dilated right atrium, a moderately dilated right ventricle, a dilated main pulmonary artery (38 mm), a mildly stenotic pulmonary artery (peak gradient=30 mmHg), and moderate-to-severe tricuspid regurgitation, with a right ventricular systolic pressure of 40 mmHg. The right atrial pacemaker lead was in its proper place, the ventricular lead in the right ventricle was undetectable due to very poor TTE views. Electrocardiography (ECG) showed a pacing rhythm with no other abnormalities (Figure 1).</p>","PeriodicalId":39149,"journal":{"name":"Journal of Tehran University Heart Center","volume":"16 2","pages":"92-94"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/9c/JTHC-16-92.PMC8742867.pdf","citationCount":"0","resultStr":"{\"title\":\"The Malposition of the Pacing Lead in the Left Ventricle through an Atrial Septal Defect.\",\"authors\":\"Arezou Zoroufian, Ali Vasheghani-Farahani, Neda Toofaninejad\",\"doi\":\"10.18502/jthc.v16i2.7393\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 54-year-old woman with a history of unknown childhood cardiac surgery underwent dual-chamber pacemaker implantation due to an advanced atrioventricular block in our center. One week later, we were asked to further evaluate tricuspid regurgitation via transthoracic echocardiography (TTE). The postoperative TTE demonstrated a left ventricular ejection fraction of 45%, as well as moderate mitral regurgitation, a severely dilated right atrium, a moderately dilated right ventricle, a dilated main pulmonary artery (38 mm), a mildly stenotic pulmonary artery (peak gradient=30 mmHg), and moderate-to-severe tricuspid regurgitation, with a right ventricular systolic pressure of 40 mmHg. The right atrial pacemaker lead was in its proper place, the ventricular lead in the right ventricle was undetectable due to very poor TTE views. Electrocardiography (ECG) showed a pacing rhythm with no other abnormalities (Figure 1).</p>\",\"PeriodicalId\":39149,\"journal\":{\"name\":\"Journal of Tehran University Heart Center\",\"volume\":\"16 2\",\"pages\":\"92-94\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/9c/JTHC-16-92.PMC8742867.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Tehran University Heart Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/jthc.v16i2.7393\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Tehran University Heart Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jthc.v16i2.7393","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
The Malposition of the Pacing Lead in the Left Ventricle through an Atrial Septal Defect.
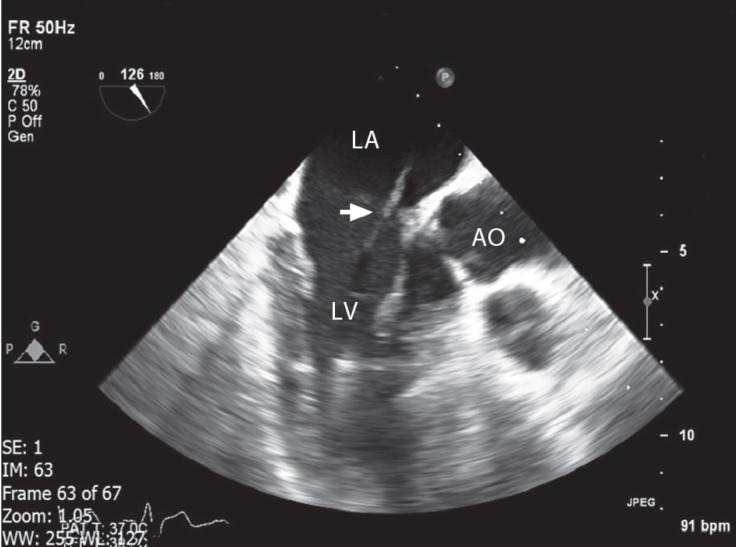
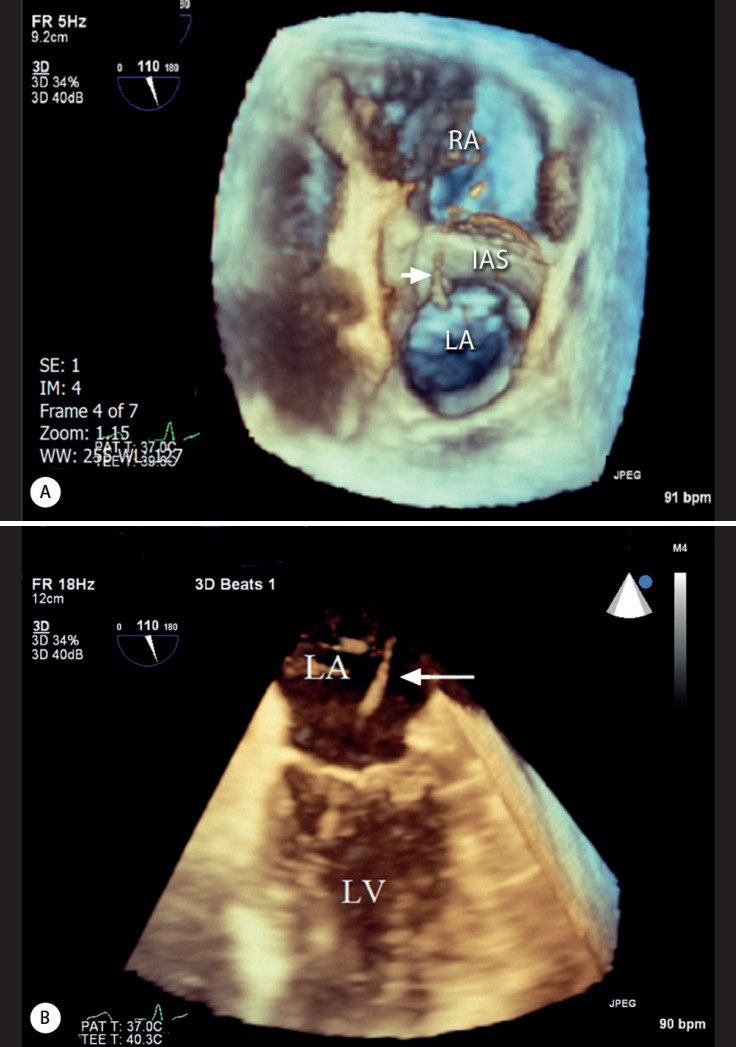
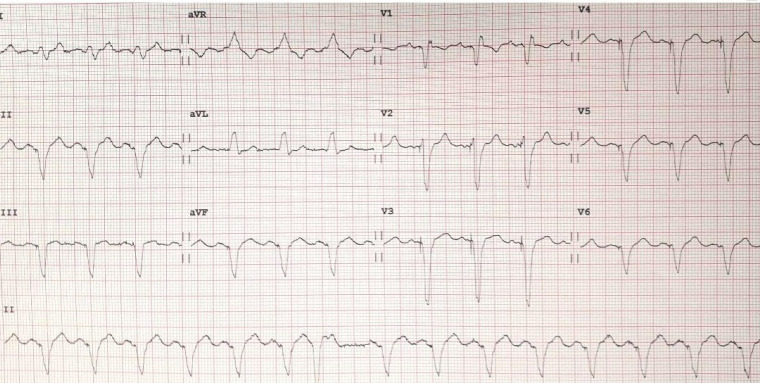
A 54-year-old woman with a history of unknown childhood cardiac surgery underwent dual-chamber pacemaker implantation due to an advanced atrioventricular block in our center. One week later, we were asked to further evaluate tricuspid regurgitation via transthoracic echocardiography (TTE). The postoperative TTE demonstrated a left ventricular ejection fraction of 45%, as well as moderate mitral regurgitation, a severely dilated right atrium, a moderately dilated right ventricle, a dilated main pulmonary artery (38 mm), a mildly stenotic pulmonary artery (peak gradient=30 mmHg), and moderate-to-severe tricuspid regurgitation, with a right ventricular systolic pressure of 40 mmHg. The right atrial pacemaker lead was in its proper place, the ventricular lead in the right ventricle was undetectable due to very poor TTE views. Electrocardiography (ECG) showed a pacing rhythm with no other abnormalities (Figure 1).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


