Zhiqi Liang, Lucy Thomas, Gwendolen Jull, Julia Treleaven
{"title":"偏头痛的颈椎肌肉骨骼损伤。","authors":"Zhiqi Liang, Lucy Thomas, Gwendolen Jull, Julia Treleaven","doi":"10.1186/s40945-021-00123-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neck pain is common and disabling amongst individuals with migraine. Cervical musculoskeletal interventions are often sought but there is currently no evidence to support such interventions for this population. Improved understanding of how cervical musculoskeletal impairments present in migraine can elucidate neck pain mechanisms and guide clinicians and researchers in the management of patients with migraine and neck pain.</p><p><strong>Main body: </strong>Migraine hypersensitivity is a major consideration when assessing for cervical impairments as it can aggravate migraine and confound findings. Current evidence of cervical impairments in migraine is limited by disregard for the different underlying causes of neck pain and possible influence of hypersensitivity. Findings of cervical musculoskeletal impairments are mixed within and across studies, indicating that different forms of neck pain are present in migraine. Some migraineurs have neck pain that is part of the migraine symptom complex and therefore exhibit little or no cervical musculoskeletal impairment. Others have a cervical source of neck pain and therefore exhibit a pattern of cervical musculoskeletal impairments akin to that of cervical disorders. The presence of cervical musculoskeletal dysfunction may or may not be related to migraine but knowledge of this is currently lacking which impacts decision making on management. Cervical musculoskeletal interventions may be indicated for migraineurs with identified cervical dysfunction but other factors requiring further clarification include determination of i) patient specific outcomes, ii) impact of co-existing migraine referred neck pain, and iii) potential moderating effects of migraine hypersensitivity on treatment efficacy.</p><p><strong>Conclusions: </strong>Physiotherapists should seek a combination of cervical impairments through skilful assessment to identify if cervical musculoskeletal dysfunction is present or not in individual patients. The relevance of cervical dysfunction to migraine and influence of co-existing migraine referred neck pain need to be established through detailed evaluation of pain behaviours and further research. Future clinical trials should define expected treatment outcomes and select individuals with cervical musculoskeletal dysfunction when investigating the efficacy of cervical musculoskeletal interventions.</p>","PeriodicalId":72290,"journal":{"name":"Archives of physiotherapy","volume":"11 1","pages":"27"},"PeriodicalIF":2.9000,"publicationDate":"2021-12-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8653561/pdf/","citationCount":"8","resultStr":"{\"title\":\"Cervical musculoskeletal impairments in migraine.\",\"authors\":\"Zhiqi Liang, Lucy Thomas, Gwendolen Jull, Julia Treleaven\",\"doi\":\"10.1186/s40945-021-00123-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neck pain is common and disabling amongst individuals with migraine. Cervical musculoskeletal interventions are often sought but there is currently no evidence to support such interventions for this population. Improved understanding of how cervical musculoskeletal impairments present in migraine can elucidate neck pain mechanisms and guide clinicians and researchers in the management of patients with migraine and neck pain.</p><p><strong>Main body: </strong>Migraine hypersensitivity is a major consideration when assessing for cervical impairments as it can aggravate migraine and confound findings. Current evidence of cervical impairments in migraine is limited by disregard for the different underlying causes of neck pain and possible influence of hypersensitivity. Findings of cervical musculoskeletal impairments are mixed within and across studies, indicating that different forms of neck pain are present in migraine. Some migraineurs have neck pain that is part of the migraine symptom complex and therefore exhibit little or no cervical musculoskeletal impairment. Others have a cervical source of neck pain and therefore exhibit a pattern of cervical musculoskeletal impairments akin to that of cervical disorders. The presence of cervical musculoskeletal dysfunction may or may not be related to migraine but knowledge of this is currently lacking which impacts decision making on management. Cervical musculoskeletal interventions may be indicated for migraineurs with identified cervical dysfunction but other factors requiring further clarification include determination of i) patient specific outcomes, ii) impact of co-existing migraine referred neck pain, and iii) potential moderating effects of migraine hypersensitivity on treatment efficacy.</p><p><strong>Conclusions: </strong>Physiotherapists should seek a combination of cervical impairments through skilful assessment to identify if cervical musculoskeletal dysfunction is present or not in individual patients. The relevance of cervical dysfunction to migraine and influence of co-existing migraine referred neck pain need to be established through detailed evaluation of pain behaviours and further research. Future clinical trials should define expected treatment outcomes and select individuals with cervical musculoskeletal dysfunction when investigating the efficacy of cervical musculoskeletal interventions.</p>\",\"PeriodicalId\":72290,\"journal\":{\"name\":\"Archives of physiotherapy\",\"volume\":\"11 1\",\"pages\":\"27\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2021-12-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8653561/pdf/\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of physiotherapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40945-021-00123-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"REHABILITATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of physiotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40945-021-00123-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
Background: Neck pain is common and disabling amongst individuals with migraine. Cervical musculoskeletal interventions are often sought but there is currently no evidence to support such interventions for this population. Improved understanding of how cervical musculoskeletal impairments present in migraine can elucidate neck pain mechanisms and guide clinicians and researchers in the management of patients with migraine and neck pain.
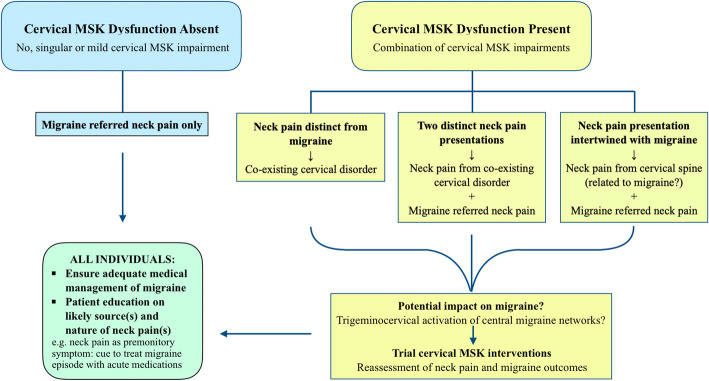
Main body: Migraine hypersensitivity is a major consideration when assessing for cervical impairments as it can aggravate migraine and confound findings. Current evidence of cervical impairments in migraine is limited by disregard for the different underlying causes of neck pain and possible influence of hypersensitivity. Findings of cervical musculoskeletal impairments are mixed within and across studies, indicating that different forms of neck pain are present in migraine. Some migraineurs have neck pain that is part of the migraine symptom complex and therefore exhibit little or no cervical musculoskeletal impairment. Others have a cervical source of neck pain and therefore exhibit a pattern of cervical musculoskeletal impairments akin to that of cervical disorders. The presence of cervical musculoskeletal dysfunction may or may not be related to migraine but knowledge of this is currently lacking which impacts decision making on management. Cervical musculoskeletal interventions may be indicated for migraineurs with identified cervical dysfunction but other factors requiring further clarification include determination of i) patient specific outcomes, ii) impact of co-existing migraine referred neck pain, and iii) potential moderating effects of migraine hypersensitivity on treatment efficacy.
Conclusions: Physiotherapists should seek a combination of cervical impairments through skilful assessment to identify if cervical musculoskeletal dysfunction is present or not in individual patients. The relevance of cervical dysfunction to migraine and influence of co-existing migraine referred neck pain need to be established through detailed evaluation of pain behaviours and further research. Future clinical trials should define expected treatment outcomes and select individuals with cervical musculoskeletal dysfunction when investigating the efficacy of cervical musculoskeletal interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


