{"title":"Carisbamate加药治疗耐药局灶性癫痫。","authors":"Chuansen Lu, Jinou Zheng, Yue Cao, Rebecca Bresnahan, Kirsty J Martin-McGill","doi":"10.1002/14651858.CD012121.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Epilepsy is one of the most common neurological disorders. Many people with epilepsy are drug-resistant and require add-on therapy, meaning that they concomitantly take multiple antiepileptic drugs. Carisbamate is a drug which is taken orally and inhibits voltage-gated sodium channels. Carisbamate may be useful for drug-resistant focal epilepsy.</p><p><strong>Objectives: </strong>To evaluate the efficacy and tolerability of carisbamate when used as an add-on therapy for drug-resistant focal epilepsy.</p><p><strong>Search methods: </strong>We searched the following databases on 8 April 2021: Cochrane Register of Studies (CRS Web) and MEDLINE (Ovid) 1946 to April 07, 2021. CRS Web includes randomised or quasi-randomised controlled trials from PubMed, Embase, ClinicalTrials.gov, WHO ICTRP, the Cochrane Central Register of Controlled Trials (CENTRAL), and the specialised registers of Cochrane review groups including Epilepsy. We also searched ongoing trials registers, checked reference lists, and contacted authors of the included trials.</p><p><strong>Selection criteria: </strong>Double-blind randomised controlled trials (RCTs) comparing carisbamate versus placebo or another antiepileptic drug, as add-on therapy for drug-resistant focal epilepsy. Trials could have a parallel-group or cross-over design.</p><p><strong>Data collection and analysis: </strong>Two review authors independently selected the trials for inclusion, assessed trial quality, and extracted data. The primary outcome was 50% or greater reduction in seizure frequency (responder rate). The secondary outcomes were: seizure freedom, treatment withdrawal (for any reason and due to adverse events); adverse events, and quality of life. We analysed data using the Mantel-Haenszel statistical method and according to the intention-to-treat population. We presented results as risk ratios (RRs) with 95% confidence intervals (CIs).</p><p><strong>Main results: </strong>We included four RCTs involving a total of 2211 participants. All four trials compared carisbamate with placebo for drug-resistant focal epilepsy. Participants in all trials were over 16 years of age and received at least one other antiepileptic drug concomitantly. We detected substantial risk of bias across the included trials. All four trials were at high risk of attrition bias due to the incomplete reporting of attrition and the high treatment withdrawal rates noted, especially with higher doses. All four trials also had unclear risk of detection bias, as they did not specify whether outcome assessors were blinded. Meta-analysis suggested that carisbamate produced a higher responder rate compared to placebo (RR 1.36, 95% CI 1.14 to 1.62; 4 studies; moderate-certainty evidence). More participants in the carsibamate group achieved seizure freedom (RR 2.43, 95% CI 0.84 to 7.03; 1 study); withdrew from treatment for any reason (RR 1.32, 95% CI 0.82 to 2.12; 4 studies); and withdrew from treatment due to adverse events (RR 1.80, 95% CI 0.78 to 4.17; 4 studies) than in the placebo group. However, the evidence for the three outcomes was very low-certainty. There was no difference between treatment groups for the proportion of participants experiencing at least one adverse event (RR 1.10, 95% CI 0.93 to 1.30; 2 studies; low-certainty evidence). More participants in the carisbamate group than in the placebo group developed dizziness (RR 2.06, 95% CI 1.23 to 3.44; 4 studies; very low-certainty evidence) and somnolence (RR 1.82, 95% CI 1.28 to 2.58; 4 studies; low-certainty evidence), but not fatigue (RR 1.11, 95% CI 0.73 to 1.68; 3 studies); headache (RR 1.13, 95% CI 0.92 to 1.38; 4 studies); or nausea (RR 1.19, 95% CI 0.81 to 1.75; 3 studies). None of the included trials reported quality of life.</p><p><strong>Authors' conclusions: </strong>The results suggest that carisbamate may demonstrate efficacy and tolerability as an add-on therapy for drug-resistant focal epilepsy. Importantly, the evidence for all outcomes except responder rate was of low to very low certainty, therefore we are uncertain of the accuracy of the reported effects. The certainty of the evidence is limited by the significant risk of bias associated with the included studies, as well as the statistical heterogeneity detected for some outcomes. Consequently, it is difficult for these findings to inform clinical practice. The studies were all of short duration and only included adult study populations. There is a need for further RCTs with more clear methodology, long-term follow-up, more clinical outcomes, more seizure types, and a broader range of participants.</p>","PeriodicalId":515753,"journal":{"name":"The Cochrane database of systematic reviews","volume":" ","pages":"CD012121"},"PeriodicalIF":0.0000,"publicationDate":"2021-12-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8647098/pdf/CD012121.pdf","citationCount":"0","resultStr":"{\"title\":\"Carisbamate add-on therapy for drug-resistant focal epilepsy.\",\"authors\":\"Chuansen Lu, Jinou Zheng, Yue Cao, Rebecca Bresnahan, Kirsty J Martin-McGill\",\"doi\":\"10.1002/14651858.CD012121.pub2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Epilepsy is one of the most common neurological disorders. Many people with epilepsy are drug-resistant and require add-on therapy, meaning that they concomitantly take multiple antiepileptic drugs. Carisbamate is a drug which is taken orally and inhibits voltage-gated sodium channels. Carisbamate may be useful for drug-resistant focal epilepsy.</p><p><strong>Objectives: </strong>To evaluate the efficacy and tolerability of carisbamate when used as an add-on therapy for drug-resistant focal epilepsy.</p><p><strong>Search methods: </strong>We searched the following databases on 8 April 2021: Cochrane Register of Studies (CRS Web) and MEDLINE (Ovid) 1946 to April 07, 2021. CRS Web includes randomised or quasi-randomised controlled trials from PubMed, Embase, ClinicalTrials.gov, WHO ICTRP, the Cochrane Central Register of Controlled Trials (CENTRAL), and the specialised registers of Cochrane review groups including Epilepsy. We also searched ongoing trials registers, checked reference lists, and contacted authors of the included trials.</p><p><strong>Selection criteria: </strong>Double-blind randomised controlled trials (RCTs) comparing carisbamate versus placebo or another antiepileptic drug, as add-on therapy for drug-resistant focal epilepsy. Trials could have a parallel-group or cross-over design.</p><p><strong>Data collection and analysis: </strong>Two review authors independently selected the trials for inclusion, assessed trial quality, and extracted data. The primary outcome was 50% or greater reduction in seizure frequency (responder rate). The secondary outcomes were: seizure freedom, treatment withdrawal (for any reason and due to adverse events); adverse events, and quality of life. We analysed data using the Mantel-Haenszel statistical method and according to the intention-to-treat population. We presented results as risk ratios (RRs) with 95% confidence intervals (CIs).</p><p><strong>Main results: </strong>We included four RCTs involving a total of 2211 participants. All four trials compared carisbamate with placebo for drug-resistant focal epilepsy. Participants in all trials were over 16 years of age and received at least one other antiepileptic drug concomitantly. We detected substantial risk of bias across the included trials. All four trials were at high risk of attrition bias due to the incomplete reporting of attrition and the high treatment withdrawal rates noted, especially with higher doses. All four trials also had unclear risk of detection bias, as they did not specify whether outcome assessors were blinded. Meta-analysis suggested that carisbamate produced a higher responder rate compared to placebo (RR 1.36, 95% CI 1.14 to 1.62; 4 studies; moderate-certainty evidence). More participants in the carsibamate group achieved seizure freedom (RR 2.43, 95% CI 0.84 to 7.03; 1 study); withdrew from treatment for any reason (RR 1.32, 95% CI 0.82 to 2.12; 4 studies); and withdrew from treatment due to adverse events (RR 1.80, 95% CI 0.78 to 4.17; 4 studies) than in the placebo group. However, the evidence for the three outcomes was very low-certainty. There was no difference between treatment groups for the proportion of participants experiencing at least one adverse event (RR 1.10, 95% CI 0.93 to 1.30; 2 studies; low-certainty evidence). More participants in the carisbamate group than in the placebo group developed dizziness (RR 2.06, 95% CI 1.23 to 3.44; 4 studies; very low-certainty evidence) and somnolence (RR 1.82, 95% CI 1.28 to 2.58; 4 studies; low-certainty evidence), but not fatigue (RR 1.11, 95% CI 0.73 to 1.68; 3 studies); headache (RR 1.13, 95% CI 0.92 to 1.38; 4 studies); or nausea (RR 1.19, 95% CI 0.81 to 1.75; 3 studies). None of the included trials reported quality of life.</p><p><strong>Authors' conclusions: </strong>The results suggest that carisbamate may demonstrate efficacy and tolerability as an add-on therapy for drug-resistant focal epilepsy. Importantly, the evidence for all outcomes except responder rate was of low to very low certainty, therefore we are uncertain of the accuracy of the reported effects. The certainty of the evidence is limited by the significant risk of bias associated with the included studies, as well as the statistical heterogeneity detected for some outcomes. Consequently, it is difficult for these findings to inform clinical practice. The studies were all of short duration and only included adult study populations. There is a need for further RCTs with more clear methodology, long-term follow-up, more clinical outcomes, more seizure types, and a broader range of participants.</p>\",\"PeriodicalId\":515753,\"journal\":{\"name\":\"The Cochrane database of systematic reviews\",\"volume\":\" \",\"pages\":\"CD012121\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-12-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8647098/pdf/CD012121.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Cochrane database of systematic reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/14651858.CD012121.pub2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cochrane database of systematic reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/14651858.CD012121.pub2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:癫痫是最常见的神经系统疾病之一。许多癫痫患者具有耐药性,需要附加治疗,这意味着他们同时服用多种抗癫痫药物。Carisbamate是一种口服药物,可抑制电压门控钠通道。Carisbamate可能对耐药局灶性癫痫有用。目的:评价carisbamate作为附加疗法治疗耐药局灶性癫痫的疗效和耐受性。检索方法:我们于2021年4月8日检索了以下数据库:Cochrane Register of Studies (CRS Web)和MEDLINE (Ovid) 1946年至2021年4月7日。CRS Web包括来自PubMed、Embase、ClinicalTrials.gov、WHO ICTRP、Cochrane中央对照试验注册库(Central)和Cochrane综述组(包括Epilepsy)的专门注册库的随机或准随机对照试验。我们还检索了正在进行的试验注册,检查了参考文献列表,并联系了纳入试验的作者。选择标准:双盲随机对照试验(rct)比较carisbamate与安慰剂或另一种抗癫痫药物,作为耐药局灶性癫痫的附加治疗。试验可以采用平行组或交叉设计。数据收集和分析:两位综述作者独立选择纳入的试验,评估试验质量,并提取数据。主要结局是癫痫发作频率(应答率)降低50%或以上。次要结局是:癫痫发作自由,治疗停药(任何原因和不良事件);不良事件和生活质量。我们使用Mantel-Haenszel统计方法并根据意向治疗人群分析数据。我们以95%置信区间(ci)的风险比(rr)来呈现结果。主要结果:我们纳入了4项随机对照试验,共涉及2211名受试者。所有四项试验都比较了carisbamate与安慰剂治疗耐药局灶性癫痫。所有试验的参与者年龄均在16岁以上,同时接受至少一种其他抗癫痫药物治疗。我们在纳入的试验中发现了显著的偏倚风险。由于消耗报告不完整和治疗停药率高,特别是高剂量,所有四项试验都有很高的消耗偏倚风险。所有四项试验也有不明确的检测偏倚风险,因为它们没有明确结果评估者是否采用盲法。荟萃分析显示,与安慰剂相比,carisbamate产生更高的应答率(RR 1.36, 95% CI 1.14至1.62;4研究;moderate-certainty证据)。carsibamate组更多的参与者获得了癫痫发作自由(RR 2.43, 95% CI 0.84 ~ 7.03;1研究);因任何原因退出治疗(RR 1.32, 95% CI 0.82 ~ 2.12;4研究);并因不良事件退出治疗(RR 1.80, 95% CI 0.78 ~ 4.17;(4项研究)比安慰剂组要多。然而,这三种结果的证据是非常不确定的。治疗组之间至少发生一次不良事件的参与者比例无差异(RR 1.10, 95% CI 0.93 ~ 1.30;2研究;确定性的证据)。carisbamate组比安慰剂组有更多的参与者出现头晕(RR 2.06, 95% CI 1.23至3.44;4研究;非常低确定性证据)和嗜睡(RR 1.82, 95% CI 1.28至2.58;4研究;低确定性证据),但没有疲劳(RR 1.11, 95% CI 0.73至1.68;3研究);头痛(RR 1.13, 95% CI 0.92 ~ 1.38;4研究);或恶心(RR 1.19, 95% CI 0.81 - 1.75;3研究)。纳入的试验均未报告生活质量。作者的结论:结果表明,carisbamate作为一种附加治疗耐药局灶性癫痫的疗效和耐受性。重要的是,除了应答率外,所有结果的证据都是低到非常低的确定性,因此我们不确定报告效果的准确性。证据的确定性受到与纳入的研究相关的显著偏倚风险的限制,以及在某些结果中检测到的统计异质性。因此,这些发现很难用于临床实践。这些研究的持续时间都很短,而且只包括成人研究人群。需要进一步的随机对照试验,更明确的方法,长期随访,更多的临床结果,更多的癫痫发作类型和更广泛的参与者。
Carisbamate add-on therapy for drug-resistant focal epilepsy.
Background: Epilepsy is one of the most common neurological disorders. Many people with epilepsy are drug-resistant and require add-on therapy, meaning that they concomitantly take multiple antiepileptic drugs. Carisbamate is a drug which is taken orally and inhibits voltage-gated sodium channels. Carisbamate may be useful for drug-resistant focal epilepsy.
Objectives: To evaluate the efficacy and tolerability of carisbamate when used as an add-on therapy for drug-resistant focal epilepsy.
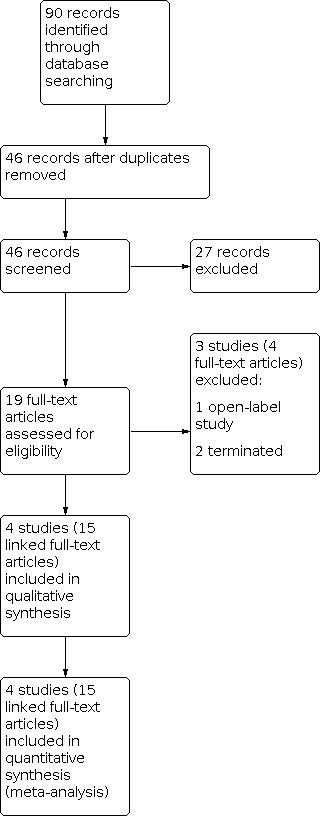
Search methods: We searched the following databases on 8 April 2021: Cochrane Register of Studies (CRS Web) and MEDLINE (Ovid) 1946 to April 07, 2021. CRS Web includes randomised or quasi-randomised controlled trials from PubMed, Embase, ClinicalTrials.gov, WHO ICTRP, the Cochrane Central Register of Controlled Trials (CENTRAL), and the specialised registers of Cochrane review groups including Epilepsy. We also searched ongoing trials registers, checked reference lists, and contacted authors of the included trials.
Selection criteria: Double-blind randomised controlled trials (RCTs) comparing carisbamate versus placebo or another antiepileptic drug, as add-on therapy for drug-resistant focal epilepsy. Trials could have a parallel-group or cross-over design.
Data collection and analysis: Two review authors independently selected the trials for inclusion, assessed trial quality, and extracted data. The primary outcome was 50% or greater reduction in seizure frequency (responder rate). The secondary outcomes were: seizure freedom, treatment withdrawal (for any reason and due to adverse events); adverse events, and quality of life. We analysed data using the Mantel-Haenszel statistical method and according to the intention-to-treat population. We presented results as risk ratios (RRs) with 95% confidence intervals (CIs).
Main results: We included four RCTs involving a total of 2211 participants. All four trials compared carisbamate with placebo for drug-resistant focal epilepsy. Participants in all trials were over 16 years of age and received at least one other antiepileptic drug concomitantly. We detected substantial risk of bias across the included trials. All four trials were at high risk of attrition bias due to the incomplete reporting of attrition and the high treatment withdrawal rates noted, especially with higher doses. All four trials also had unclear risk of detection bias, as they did not specify whether outcome assessors were blinded. Meta-analysis suggested that carisbamate produced a higher responder rate compared to placebo (RR 1.36, 95% CI 1.14 to 1.62; 4 studies; moderate-certainty evidence). More participants in the carsibamate group achieved seizure freedom (RR 2.43, 95% CI 0.84 to 7.03; 1 study); withdrew from treatment for any reason (RR 1.32, 95% CI 0.82 to 2.12; 4 studies); and withdrew from treatment due to adverse events (RR 1.80, 95% CI 0.78 to 4.17; 4 studies) than in the placebo group. However, the evidence for the three outcomes was very low-certainty. There was no difference between treatment groups for the proportion of participants experiencing at least one adverse event (RR 1.10, 95% CI 0.93 to 1.30; 2 studies; low-certainty evidence). More participants in the carisbamate group than in the placebo group developed dizziness (RR 2.06, 95% CI 1.23 to 3.44; 4 studies; very low-certainty evidence) and somnolence (RR 1.82, 95% CI 1.28 to 2.58; 4 studies; low-certainty evidence), but not fatigue (RR 1.11, 95% CI 0.73 to 1.68; 3 studies); headache (RR 1.13, 95% CI 0.92 to 1.38; 4 studies); or nausea (RR 1.19, 95% CI 0.81 to 1.75; 3 studies). None of the included trials reported quality of life.
Authors' conclusions: The results suggest that carisbamate may demonstrate efficacy and tolerability as an add-on therapy for drug-resistant focal epilepsy. Importantly, the evidence for all outcomes except responder rate was of low to very low certainty, therefore we are uncertain of the accuracy of the reported effects. The certainty of the evidence is limited by the significant risk of bias associated with the included studies, as well as the statistical heterogeneity detected for some outcomes. Consequently, it is difficult for these findings to inform clinical practice. The studies were all of short duration and only included adult study populations. There is a need for further RCTs with more clear methodology, long-term follow-up, more clinical outcomes, more seizure types, and a broader range of participants.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


