Vasileios Kontogiannis, Diarmuid Coughlan, Mehdi Javanbakht, Patience Kunonga, Fiona Beyer, Catherine Richmond, Andy Bryant, Dalvir Bajwa, Robert A Ellis, Luke Vale
{"title":"原发性肿瘤切除后早期皮肤黑色素瘤的最佳监测策略:经济评估。","authors":"Vasileios Kontogiannis, Diarmuid Coughlan, Mehdi Javanbakht, Patience Kunonga, Fiona Beyer, Catherine Richmond, Andy Bryant, Dalvir Bajwa, Robert A Ellis, Luke Vale","doi":"10.1177/23814683211069988","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background.</b> Consensus on standardized active surveillance or follow-up care by clinicians is lacking leading to considerable variation in practice across countries. An important structural modelling consideration is that self-examination by patients and their partners can detect melanoma recurrence outside of active surveillance regimes. <b>Objectives.</b> To identify candidate melanoma surveillance strategies for American Joint Committee on Cancer (AJCC) stage I disease and compare them with the current recommended practice in a cost-utility analysis framework. <b>Methods.</b> In consultation with UK clinical experts, a microsimulation model was built in TreeAge Pro 2019 R1.0 (Williamstown, MA, USA) to evaluate surveillance strategies for AJCC stage IA and IB melanoma patients separately. The model incorporated patient behaviors such as self-detection and emergency visits to examine suspicious lesions. A National Health Service (NHS) perspective was taken. Model input parameters were taken from the literature and where data were not available, local expert opinion was sought. Probabilistic sensitivity analysis, one-way sensitivity analysis on pertinent parameters and value of information was performed. <b>Results.</b> In the base-case probabilistic sensitivity analysis, less intensive surveillance strategies for AJCC stage IA and IB had lower total lifetime costs than the current National Institute for Health and Care Excellence (NICE) recommended strategy with similar effectiveness in terms of quality-adjusted life years and thereby likely to be cost-effective. Many strategies had similar effectiveness due to the relatively low chance of recurrence and the high rate of self-detection. Sensitivity and scenario analyses did not change these findings. <b>Conclusions.</b> Our model findings suggest that less resource intensive surveillance may be cost-effective compared with the current NICE surveillance guidelines. However, to advocate convincingly for changes, better evidence is required.</p>","PeriodicalId":520707,"journal":{"name":"MDM policy & practice","volume":" ","pages":"23814683211069988"},"PeriodicalIF":1.7000,"publicationDate":"2022-01-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d3/f1/10.1177_23814683211069988.PMC8743969.pdf","citationCount":"0","resultStr":"{\"title\":\"Optimal Surveillance Strategies for Early-Stage Cutaneous Melanoma Post Primary Tumor Excision: An Economic Evaluation.\",\"authors\":\"Vasileios Kontogiannis, Diarmuid Coughlan, Mehdi Javanbakht, Patience Kunonga, Fiona Beyer, Catherine Richmond, Andy Bryant, Dalvir Bajwa, Robert A Ellis, Luke Vale\",\"doi\":\"10.1177/23814683211069988\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background.</b> Consensus on standardized active surveillance or follow-up care by clinicians is lacking leading to considerable variation in practice across countries. An important structural modelling consideration is that self-examination by patients and their partners can detect melanoma recurrence outside of active surveillance regimes. <b>Objectives.</b> To identify candidate melanoma surveillance strategies for American Joint Committee on Cancer (AJCC) stage I disease and compare them with the current recommended practice in a cost-utility analysis framework. <b>Methods.</b> In consultation with UK clinical experts, a microsimulation model was built in TreeAge Pro 2019 R1.0 (Williamstown, MA, USA) to evaluate surveillance strategies for AJCC stage IA and IB melanoma patients separately. The model incorporated patient behaviors such as self-detection and emergency visits to examine suspicious lesions. A National Health Service (NHS) perspective was taken. Model input parameters were taken from the literature and where data were not available, local expert opinion was sought. Probabilistic sensitivity analysis, one-way sensitivity analysis on pertinent parameters and value of information was performed. <b>Results.</b> In the base-case probabilistic sensitivity analysis, less intensive surveillance strategies for AJCC stage IA and IB had lower total lifetime costs than the current National Institute for Health and Care Excellence (NICE) recommended strategy with similar effectiveness in terms of quality-adjusted life years and thereby likely to be cost-effective. Many strategies had similar effectiveness due to the relatively low chance of recurrence and the high rate of self-detection. Sensitivity and scenario analyses did not change these findings. <b>Conclusions.</b> Our model findings suggest that less resource intensive surveillance may be cost-effective compared with the current NICE surveillance guidelines. However, to advocate convincingly for changes, better evidence is required.</p>\",\"PeriodicalId\":520707,\"journal\":{\"name\":\"MDM policy & practice\",\"volume\":\" \",\"pages\":\"23814683211069988\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-01-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d3/f1/10.1177_23814683211069988.PMC8743969.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"MDM policy & practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23814683211069988\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM policy & practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683211069988","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景。由于缺乏对标准化主动监测或临床医生随访护理的共识,导致各国在实践中存在相当大的差异。一个重要的结构建模考虑因素是患者及其伴侣的自我检查可以在主动监测制度之外发现黑色素瘤复发。目标。确定美国癌症联合委员会(AJCC) I期疾病的候选黑色素瘤监测策略,并在成本效用分析框架中将其与当前推荐的做法进行比较。方法。在与英国临床专家协商后,在TreeAge Pro 2019 R1.0 (Williamstown, MA, USA)中建立了微模拟模型,分别评估AJCC IA期和IB期黑色素瘤患者的监测策略。该模型结合了患者的行为,如自我检测和急诊检查可疑病变。采取了国民保健服务(NHS)的观点。模型输入参数取自文献,如果没有可用的数据,则寻求当地专家的意见。对相关参数和信息值进行了概率敏感性分析、单向敏感性分析。结果。在基本情况概率敏感性分析中,AJCC IA期和IB期较低强度的监测策略比目前国家健康与护理卓越研究所(NICE)推荐的策略具有更低的总生命周期成本,在质量调整生命年方面具有相似的有效性,因此可能具有成本效益。由于相对较低的复发率和较高的自检率,许多策略具有相似的效果。敏感性和情景分析没有改变这些发现。结论。我们的模型结果表明,与目前的NICE监测指南相比,资源密集程度较低的监测可能更具成本效益。然而,要令人信服地倡导变革,还需要更好的证据。
Optimal Surveillance Strategies for Early-Stage Cutaneous Melanoma Post Primary Tumor Excision: An Economic Evaluation.
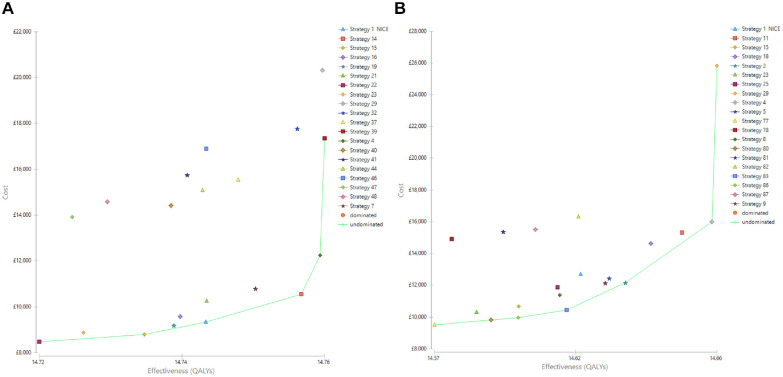
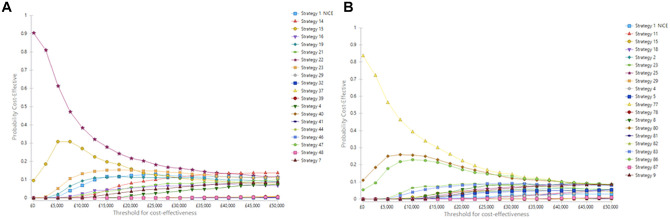
Background. Consensus on standardized active surveillance or follow-up care by clinicians is lacking leading to considerable variation in practice across countries. An important structural modelling consideration is that self-examination by patients and their partners can detect melanoma recurrence outside of active surveillance regimes. Objectives. To identify candidate melanoma surveillance strategies for American Joint Committee on Cancer (AJCC) stage I disease and compare them with the current recommended practice in a cost-utility analysis framework. Methods. In consultation with UK clinical experts, a microsimulation model was built in TreeAge Pro 2019 R1.0 (Williamstown, MA, USA) to evaluate surveillance strategies for AJCC stage IA and IB melanoma patients separately. The model incorporated patient behaviors such as self-detection and emergency visits to examine suspicious lesions. A National Health Service (NHS) perspective was taken. Model input parameters were taken from the literature and where data were not available, local expert opinion was sought. Probabilistic sensitivity analysis, one-way sensitivity analysis on pertinent parameters and value of information was performed. Results. In the base-case probabilistic sensitivity analysis, less intensive surveillance strategies for AJCC stage IA and IB had lower total lifetime costs than the current National Institute for Health and Care Excellence (NICE) recommended strategy with similar effectiveness in terms of quality-adjusted life years and thereby likely to be cost-effective. Many strategies had similar effectiveness due to the relatively low chance of recurrence and the high rate of self-detection. Sensitivity and scenario analyses did not change these findings. Conclusions. Our model findings suggest that less resource intensive surveillance may be cost-effective compared with the current NICE surveillance guidelines. However, to advocate convincingly for changes, better evidence is required.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


