Courtney D Hall, Susan J Herdman, Susan L Whitney, Eric R Anson, Wendy J Carender, Carrie W Hoppes, Stephen P Cass, Jennifer B Christy, Helen S Cohen, Terry D Fife, Joseph M Furman, Neil T Shepard, Richard A Clendaniel, J Donald Dishman, Joel A Goebel, Dara Meldrum, Cynthia Ryan, Richard L Wallace, Nakia J Woodward
{"title":"外周前庭功能障碍的前庭康复:来自美国物理治疗协会神经物理治疗学会的最新临床实践指南。","authors":"Courtney D Hall, Susan J Herdman, Susan L Whitney, Eric R Anson, Wendy J Carender, Carrie W Hoppes, Stephen P Cass, Jennifer B Christy, Helen S Cohen, Terry D Fife, Joseph M Furman, Neil T Shepard, Richard A Clendaniel, J Donald Dishman, Joel A Goebel, Dara Meldrum, Cynthia Ryan, Richard L Wallace, Nakia J Woodward","doi":"10.1097/NPT.0000000000000382","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Uncompensated vestibular hypofunction can result in symptoms of dizziness, imbalance, and/or oscillopsia, gaze and gait instability, and impaired navigation and spatial orientation; thus, may negatively impact an individual's quality of life, ability to perform activities of daily living, drive, and work. It is estimated that one-third of adults in the United States have vestibular dysfunction and the incidence increases with age. There is strong evidence supporting vestibular physical therapy for reducing symptoms, improving gaze and postural stability, and improving function in individuals with vestibular hypofunction. The purpose of this revised clinical practice guideline is to improve quality of care and outcomes for individuals with acute, subacute, and chronic unilateral and bilateral vestibular hypofunction by providing evidence-based recommendations regarding appropriate exercises.</p><p><strong>Methods: </strong>These guidelines are a revision of the 2016 guidelines and involved a systematic review of the literature published since 2015 through June 2020 across 6 databases. Article types included meta-analyses, systematic reviews, randomized controlled trials, cohort studies, case-control series, and case series for human subjects, published in English. Sixty-seven articles were identified as relevant to this clinical practice guideline and critically appraised for level of evidence.</p><p><strong>Results: </strong>Based on strong evidence, clinicians should offer vestibular rehabilitation to adults with unilateral and bilateral vestibular hypofunction who present with impairments, activity limitations, and participation restrictions related to the vestibular deficit. Based on strong evidence and a preponderance of harm over benefit, clinicians should not include voluntary saccadic or smooth-pursuit eye movements in isolation (ie, without head movement) to promote gaze stability. Based on moderate to strong evidence, clinicians may offer specific exercise techniques to target identified activity limitations and participation restrictions, including virtual reality or augmented sensory feedback. Based on strong evidence and in consideration of patient preference, clinicians should offer supervised vestibular rehabilitation. Based on moderate to weak evidence, clinicians may prescribe weekly clinic visits plus a home exercise program of gaze stabilization exercises consisting of a minimum of: (1) 3 times per day for a total of at least 12 minutes daily for individuals with acute/subacute unilateral vestibular hypofunction; (2) 3 to 5 times per day for a total of at least 20 minutes daily for 4 to 6 weeks for individuals with chronic unilateral vestibular hypofunction; (3) 3 to 5 times per day for a total of 20 to 40 minutes daily for approximately 5 to 7 weeks for individuals with bilateral vestibular hypofunction. Based on moderate evidence, clinicians may prescribe static and dynamic balance exercises for a minimum of 20 minutes daily for at least 4 to 6 weeks for individuals with chronic unilateral vestibular hypofunction and, based on expert opinion, for a minimum of 6 to 9 weeks for individuals with bilateral vestibular hypofunction. Based on moderate evidence, clinicians may use achievement of primary goals, resolution of symptoms, normalized balance and vestibular function, or plateau in progress as reasons for stopping therapy. Based on moderate to strong evidence, clinicians may evaluate factors, including time from onset of symptoms, comorbidities, cognitive function, and use of medication that could modify rehabilitation outcomes.</p><p><strong>Discussion: </strong>Recent evidence supports the original recommendations from the 2016 guidelines. There is strong evidence that vestibular physical therapy provides a clear and substantial benefit to individuals with unilateral and bilateral vestibular hypofunction.</p><p><strong>Limitations: </strong>The focus of the guideline was on peripheral vestibular hypofunction; thus, the recommendations of the guideline may not apply to individuals with central vestibular disorders. One criterion for study inclusion was that vestibular hypofunction was determined based on objective vestibular function tests. This guideline may not apply to individuals who report symptoms of dizziness, imbalance, and/or oscillopsia without a diagnosis of vestibular hypofunction.</p><p><strong>Disclaimer: </strong>These recommendations are intended as a guide to optimize rehabilitation outcomes for individuals undergoing vestibular physical therapy. The contents of this guideline were developed with support from the American Physical Therapy Association and the Academy of Neurologic Physical Therapy using a rigorous review process. The authors declared no conflict of interest and maintained editorial independence.Video Abstract available for more insights from the authors (see the Video, Supplemental Digital Content 1, available at: http://links.lww.com/JNPT/A369).</p>","PeriodicalId":49030,"journal":{"name":"Journal of Neurologic Physical Therapy","volume":null,"pages":null},"PeriodicalIF":2.6000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/36/jnpt-46-118.PMC8920012.pdf","citationCount":"62","resultStr":"{\"title\":\"Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association.\",\"authors\":\"Courtney D Hall, Susan J Herdman, Susan L Whitney, Eric R Anson, Wendy J Carender, Carrie W Hoppes, Stephen P Cass, Jennifer B Christy, Helen S Cohen, Terry D Fife, Joseph M Furman, Neil T Shepard, Richard A Clendaniel, J Donald Dishman, Joel A Goebel, Dara Meldrum, Cynthia Ryan, Richard L Wallace, Nakia J Woodward\",\"doi\":\"10.1097/NPT.0000000000000382\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Uncompensated vestibular hypofunction can result in symptoms of dizziness, imbalance, and/or oscillopsia, gaze and gait instability, and impaired navigation and spatial orientation; thus, may negatively impact an individual's quality of life, ability to perform activities of daily living, drive, and work. It is estimated that one-third of adults in the United States have vestibular dysfunction and the incidence increases with age. There is strong evidence supporting vestibular physical therapy for reducing symptoms, improving gaze and postural stability, and improving function in individuals with vestibular hypofunction. The purpose of this revised clinical practice guideline is to improve quality of care and outcomes for individuals with acute, subacute, and chronic unilateral and bilateral vestibular hypofunction by providing evidence-based recommendations regarding appropriate exercises.</p><p><strong>Methods: </strong>These guidelines are a revision of the 2016 guidelines and involved a systematic review of the literature published since 2015 through June 2020 across 6 databases. Article types included meta-analyses, systematic reviews, randomized controlled trials, cohort studies, case-control series, and case series for human subjects, published in English. Sixty-seven articles were identified as relevant to this clinical practice guideline and critically appraised for level of evidence.</p><p><strong>Results: </strong>Based on strong evidence, clinicians should offer vestibular rehabilitation to adults with unilateral and bilateral vestibular hypofunction who present with impairments, activity limitations, and participation restrictions related to the vestibular deficit. Based on strong evidence and a preponderance of harm over benefit, clinicians should not include voluntary saccadic or smooth-pursuit eye movements in isolation (ie, without head movement) to promote gaze stability. Based on moderate to strong evidence, clinicians may offer specific exercise techniques to target identified activity limitations and participation restrictions, including virtual reality or augmented sensory feedback. Based on strong evidence and in consideration of patient preference, clinicians should offer supervised vestibular rehabilitation. Based on moderate to weak evidence, clinicians may prescribe weekly clinic visits plus a home exercise program of gaze stabilization exercises consisting of a minimum of: (1) 3 times per day for a total of at least 12 minutes daily for individuals with acute/subacute unilateral vestibular hypofunction; (2) 3 to 5 times per day for a total of at least 20 minutes daily for 4 to 6 weeks for individuals with chronic unilateral vestibular hypofunction; (3) 3 to 5 times per day for a total of 20 to 40 minutes daily for approximately 5 to 7 weeks for individuals with bilateral vestibular hypofunction. Based on moderate evidence, clinicians may prescribe static and dynamic balance exercises for a minimum of 20 minutes daily for at least 4 to 6 weeks for individuals with chronic unilateral vestibular hypofunction and, based on expert opinion, for a minimum of 6 to 9 weeks for individuals with bilateral vestibular hypofunction. Based on moderate evidence, clinicians may use achievement of primary goals, resolution of symptoms, normalized balance and vestibular function, or plateau in progress as reasons for stopping therapy. Based on moderate to strong evidence, clinicians may evaluate factors, including time from onset of symptoms, comorbidities, cognitive function, and use of medication that could modify rehabilitation outcomes.</p><p><strong>Discussion: </strong>Recent evidence supports the original recommendations from the 2016 guidelines. There is strong evidence that vestibular physical therapy provides a clear and substantial benefit to individuals with unilateral and bilateral vestibular hypofunction.</p><p><strong>Limitations: </strong>The focus of the guideline was on peripheral vestibular hypofunction; thus, the recommendations of the guideline may not apply to individuals with central vestibular disorders. One criterion for study inclusion was that vestibular hypofunction was determined based on objective vestibular function tests. This guideline may not apply to individuals who report symptoms of dizziness, imbalance, and/or oscillopsia without a diagnosis of vestibular hypofunction.</p><p><strong>Disclaimer: </strong>These recommendations are intended as a guide to optimize rehabilitation outcomes for individuals undergoing vestibular physical therapy. The contents of this guideline were developed with support from the American Physical Therapy Association and the Academy of Neurologic Physical Therapy using a rigorous review process. The authors declared no conflict of interest and maintained editorial independence.Video Abstract available for more insights from the authors (see the Video, Supplemental Digital Content 1, available at: http://links.lww.com/JNPT/A369).</p>\",\"PeriodicalId\":49030,\"journal\":{\"name\":\"Journal of Neurologic Physical Therapy\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2022-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/36/jnpt-46-118.PMC8920012.pdf\",\"citationCount\":\"62\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurologic Physical Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/NPT.0000000000000382\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurologic Physical Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/NPT.0000000000000382","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association.
Background: Uncompensated vestibular hypofunction can result in symptoms of dizziness, imbalance, and/or oscillopsia, gaze and gait instability, and impaired navigation and spatial orientation; thus, may negatively impact an individual's quality of life, ability to perform activities of daily living, drive, and work. It is estimated that one-third of adults in the United States have vestibular dysfunction and the incidence increases with age. There is strong evidence supporting vestibular physical therapy for reducing symptoms, improving gaze and postural stability, and improving function in individuals with vestibular hypofunction. The purpose of this revised clinical practice guideline is to improve quality of care and outcomes for individuals with acute, subacute, and chronic unilateral and bilateral vestibular hypofunction by providing evidence-based recommendations regarding appropriate exercises.
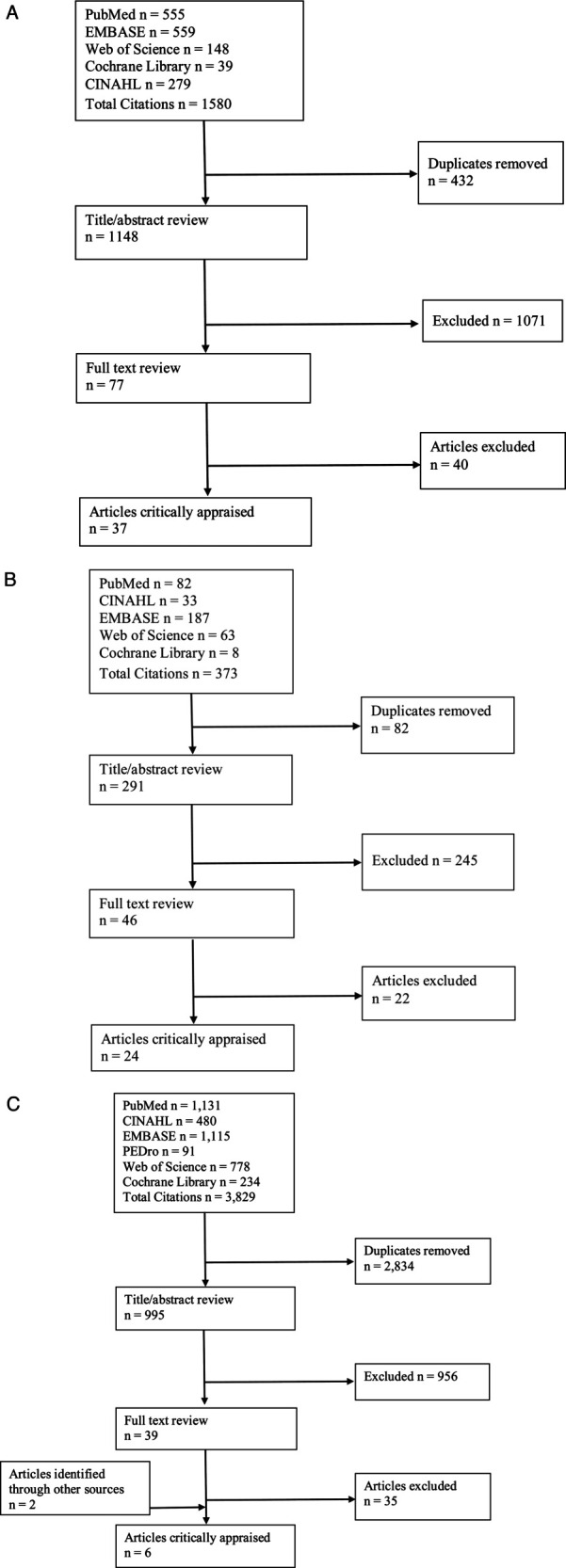
Methods: These guidelines are a revision of the 2016 guidelines and involved a systematic review of the literature published since 2015 through June 2020 across 6 databases. Article types included meta-analyses, systematic reviews, randomized controlled trials, cohort studies, case-control series, and case series for human subjects, published in English. Sixty-seven articles were identified as relevant to this clinical practice guideline and critically appraised for level of evidence.
Results: Based on strong evidence, clinicians should offer vestibular rehabilitation to adults with unilateral and bilateral vestibular hypofunction who present with impairments, activity limitations, and participation restrictions related to the vestibular deficit. Based on strong evidence and a preponderance of harm over benefit, clinicians should not include voluntary saccadic or smooth-pursuit eye movements in isolation (ie, without head movement) to promote gaze stability. Based on moderate to strong evidence, clinicians may offer specific exercise techniques to target identified activity limitations and participation restrictions, including virtual reality or augmented sensory feedback. Based on strong evidence and in consideration of patient preference, clinicians should offer supervised vestibular rehabilitation. Based on moderate to weak evidence, clinicians may prescribe weekly clinic visits plus a home exercise program of gaze stabilization exercises consisting of a minimum of: (1) 3 times per day for a total of at least 12 minutes daily for individuals with acute/subacute unilateral vestibular hypofunction; (2) 3 to 5 times per day for a total of at least 20 minutes daily for 4 to 6 weeks for individuals with chronic unilateral vestibular hypofunction; (3) 3 to 5 times per day for a total of 20 to 40 minutes daily for approximately 5 to 7 weeks for individuals with bilateral vestibular hypofunction. Based on moderate evidence, clinicians may prescribe static and dynamic balance exercises for a minimum of 20 minutes daily for at least 4 to 6 weeks for individuals with chronic unilateral vestibular hypofunction and, based on expert opinion, for a minimum of 6 to 9 weeks for individuals with bilateral vestibular hypofunction. Based on moderate evidence, clinicians may use achievement of primary goals, resolution of symptoms, normalized balance and vestibular function, or plateau in progress as reasons for stopping therapy. Based on moderate to strong evidence, clinicians may evaluate factors, including time from onset of symptoms, comorbidities, cognitive function, and use of medication that could modify rehabilitation outcomes.
Discussion: Recent evidence supports the original recommendations from the 2016 guidelines. There is strong evidence that vestibular physical therapy provides a clear and substantial benefit to individuals with unilateral and bilateral vestibular hypofunction.
Limitations: The focus of the guideline was on peripheral vestibular hypofunction; thus, the recommendations of the guideline may not apply to individuals with central vestibular disorders. One criterion for study inclusion was that vestibular hypofunction was determined based on objective vestibular function tests. This guideline may not apply to individuals who report symptoms of dizziness, imbalance, and/or oscillopsia without a diagnosis of vestibular hypofunction.
Disclaimer: These recommendations are intended as a guide to optimize rehabilitation outcomes for individuals undergoing vestibular physical therapy. The contents of this guideline were developed with support from the American Physical Therapy Association and the Academy of Neurologic Physical Therapy using a rigorous review process. The authors declared no conflict of interest and maintained editorial independence.Video Abstract available for more insights from the authors (see the Video, Supplemental Digital Content 1, available at: http://links.lww.com/JNPT/A369).
期刊介绍:
The Journal of Neurologic Physical Therapy (JNPT) is an indexed resource for dissemination of research-based evidence related to neurologic physical therapy intervention. High standards of quality are maintained through a rigorous, double-blinded, peer-review process and adherence to standards recommended by the International Committee of Medical Journal Editors. With an international editorial board made up of preeminent researchers and clinicians, JNPT publishes articles of global relevance for examination, evaluation, prognosis, intervention, and outcomes for individuals with movement deficits due to neurologic conditions. Through systematic reviews, research articles, case studies, and clinical perspectives, JNPT promotes the integration of evidence into theory, education, research, and practice of neurologic physical therapy, spanning the continuum from pathophysiology to societal participation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


