{"title":"防止国家痴呆指南建议中的歧视:一项系统综述。","authors":"Tiffeny James, Naaheed Mukadam, Andrew Sommerlad, Hossein Rostami Pour, Melanie Knowles, Ignacia Azocar, Gill Livingston","doi":"10.1371/journal.pmed.1003860","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>National dementia guidelines provide recommendations about the most effective approaches to diagnosis and interventions. Guidelines can improve care, but some groups such as people with minority characteristics may be disadvantaged if recommended approaches are the same for everyone. It is not known if dementia guidelines address specific needs related to patient characteristics. The objectives of this review are to identify which countries have national guidelines for dementia and synthesise recommendations relating to protected characteristics, as defined in the UK Equality Act 2010: age, disability, gender identity, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex, and sexual orientation.</p><p><strong>Methods and findings: </strong>We searched CINAHL, PsycINFO, and Medline databases and the Guideline International Network library from inception to March 4, 2020, for dementia guidelines in any language. We also searched, between April and September 2020, Google and the national health websites of all 196 countries in English and in each country's official languages. To be included, guidelines had to provide recommendations about dementia, which were expected to be followed by healthcare workers and be approved at a national policy level. We rated quality according to the iCAHE guideline quality checklist. We provide a narrative synthesis of recommendations identified for each protected characteristic, prioritising those from higher-quality guidelines. Forty-six guidelines from 44 countries met our criteria, of which 18 were rated as higher quality. Most guidelines (39/46; 85%) made at least one reference to protected characteristics, and we identified recommendations relating to age, disability, race (or culture, ethnicity, or language), religion, sex, and sexual orientation. Age was the most frequently referenced characteristic (31/46; 67%) followed by race (or culture, ethnicity, or language; 25/46; 54%). Recommendations included specialist investigation and support for younger people affected by dementia and consideration of culture when assessing whether someone had dementia and providing person-centred care. Guidelines recommended considering religion when providing person-centred and end-of-life care. For disability, it was recommended that healthcare workers consider intellectual disability and sensory impairment when assessing for dementia. Most recommendations related to sex recommended not using sex hormones to treat cognitive impairment in men and women. One guideline made one recommendation related to sexual orientation. The main limitation of this study is that we only included national guidelines applicable to a whole country meaning guidelines from countries with differing healthcare systems within the country may have been excluded.</p><p><strong>Conclusions: </strong>National guidelines for dementia vary in their consideration of protected characteristics. We found that around a fifth of the world's countries have guidelines for dementia. We have identified areas of good practice that can be considered for future guidelines and suggest that all guidelines provide specific evidence-based recommendations for minority groups with examples of how to implement them. This will promote equity in the care of people affected by dementia and help to ensure that people with protected characteristics also have high-quality clinical services.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 1","pages":"e1003860"},"PeriodicalIF":9.9000,"publicationDate":"2022-01-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8752020/pdf/","citationCount":"4","resultStr":"{\"title\":\"Protection against discrimination in national dementia guideline recommendations: A systematic review.\",\"authors\":\"Tiffeny James, Naaheed Mukadam, Andrew Sommerlad, Hossein Rostami Pour, Melanie Knowles, Ignacia Azocar, Gill Livingston\",\"doi\":\"10.1371/journal.pmed.1003860\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>National dementia guidelines provide recommendations about the most effective approaches to diagnosis and interventions. Guidelines can improve care, but some groups such as people with minority characteristics may be disadvantaged if recommended approaches are the same for everyone. It is not known if dementia guidelines address specific needs related to patient characteristics. The objectives of this review are to identify which countries have national guidelines for dementia and synthesise recommendations relating to protected characteristics, as defined in the UK Equality Act 2010: age, disability, gender identity, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex, and sexual orientation.</p><p><strong>Methods and findings: </strong>We searched CINAHL, PsycINFO, and Medline databases and the Guideline International Network library from inception to March 4, 2020, for dementia guidelines in any language. We also searched, between April and September 2020, Google and the national health websites of all 196 countries in English and in each country's official languages. To be included, guidelines had to provide recommendations about dementia, which were expected to be followed by healthcare workers and be approved at a national policy level. We rated quality according to the iCAHE guideline quality checklist. We provide a narrative synthesis of recommendations identified for each protected characteristic, prioritising those from higher-quality guidelines. Forty-six guidelines from 44 countries met our criteria, of which 18 were rated as higher quality. Most guidelines (39/46; 85%) made at least one reference to protected characteristics, and we identified recommendations relating to age, disability, race (or culture, ethnicity, or language), religion, sex, and sexual orientation. Age was the most frequently referenced characteristic (31/46; 67%) followed by race (or culture, ethnicity, or language; 25/46; 54%). Recommendations included specialist investigation and support for younger people affected by dementia and consideration of culture when assessing whether someone had dementia and providing person-centred care. Guidelines recommended considering religion when providing person-centred and end-of-life care. For disability, it was recommended that healthcare workers consider intellectual disability and sensory impairment when assessing for dementia. Most recommendations related to sex recommended not using sex hormones to treat cognitive impairment in men and women. One guideline made one recommendation related to sexual orientation. The main limitation of this study is that we only included national guidelines applicable to a whole country meaning guidelines from countries with differing healthcare systems within the country may have been excluded.</p><p><strong>Conclusions: </strong>National guidelines for dementia vary in their consideration of protected characteristics. We found that around a fifth of the world's countries have guidelines for dementia. We have identified areas of good practice that can be considered for future guidelines and suggest that all guidelines provide specific evidence-based recommendations for minority groups with examples of how to implement them. This will promote equity in the care of people affected by dementia and help to ensure that people with protected characteristics also have high-quality clinical services.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 1\",\"pages\":\"e1003860\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2022-01-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8752020/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003860\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003860","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Protection against discrimination in national dementia guideline recommendations: A systematic review.
Background: National dementia guidelines provide recommendations about the most effective approaches to diagnosis and interventions. Guidelines can improve care, but some groups such as people with minority characteristics may be disadvantaged if recommended approaches are the same for everyone. It is not known if dementia guidelines address specific needs related to patient characteristics. The objectives of this review are to identify which countries have national guidelines for dementia and synthesise recommendations relating to protected characteristics, as defined in the UK Equality Act 2010: age, disability, gender identity, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex, and sexual orientation.
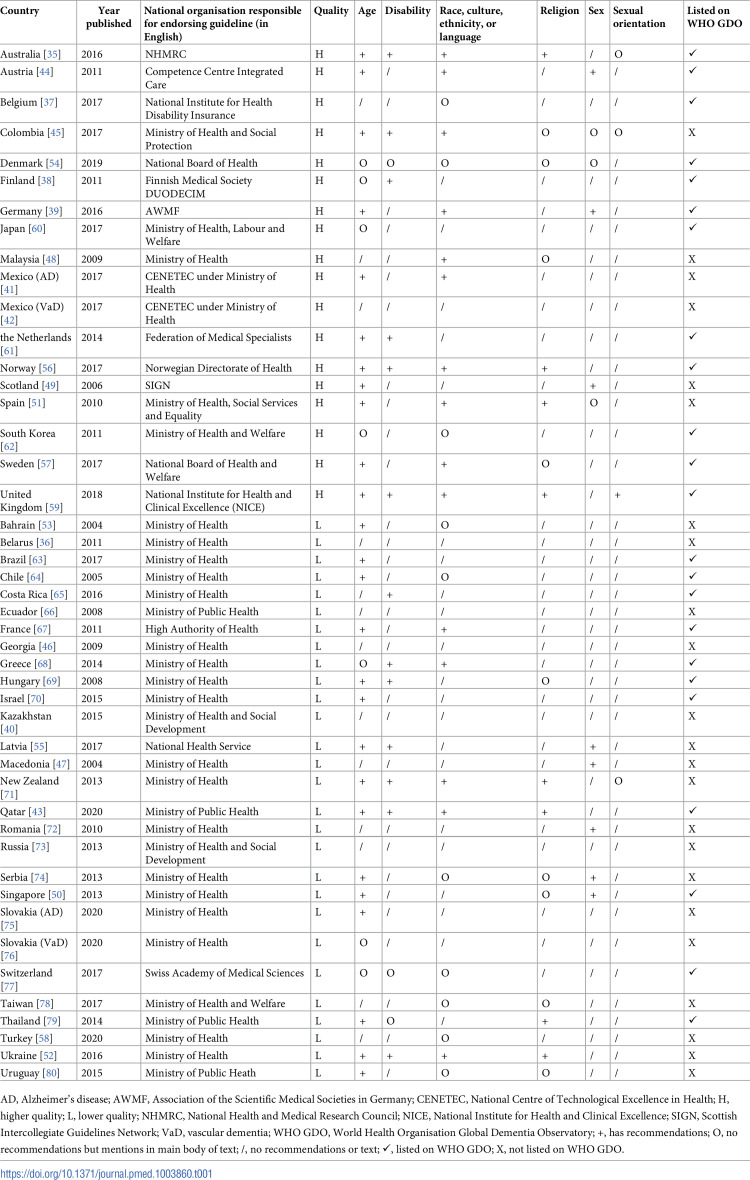
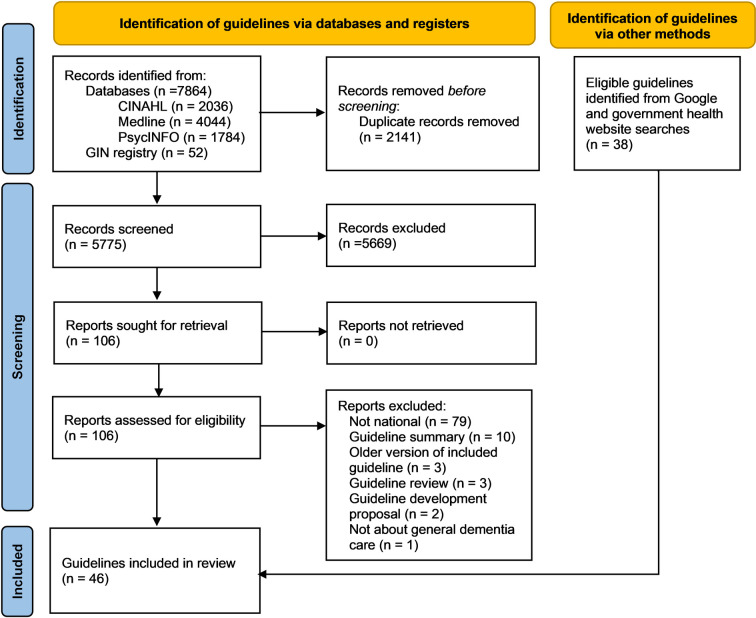
Methods and findings: We searched CINAHL, PsycINFO, and Medline databases and the Guideline International Network library from inception to March 4, 2020, for dementia guidelines in any language. We also searched, between April and September 2020, Google and the national health websites of all 196 countries in English and in each country's official languages. To be included, guidelines had to provide recommendations about dementia, which were expected to be followed by healthcare workers and be approved at a national policy level. We rated quality according to the iCAHE guideline quality checklist. We provide a narrative synthesis of recommendations identified for each protected characteristic, prioritising those from higher-quality guidelines. Forty-six guidelines from 44 countries met our criteria, of which 18 were rated as higher quality. Most guidelines (39/46; 85%) made at least one reference to protected characteristics, and we identified recommendations relating to age, disability, race (or culture, ethnicity, or language), religion, sex, and sexual orientation. Age was the most frequently referenced characteristic (31/46; 67%) followed by race (or culture, ethnicity, or language; 25/46; 54%). Recommendations included specialist investigation and support for younger people affected by dementia and consideration of culture when assessing whether someone had dementia and providing person-centred care. Guidelines recommended considering religion when providing person-centred and end-of-life care. For disability, it was recommended that healthcare workers consider intellectual disability and sensory impairment when assessing for dementia. Most recommendations related to sex recommended not using sex hormones to treat cognitive impairment in men and women. One guideline made one recommendation related to sexual orientation. The main limitation of this study is that we only included national guidelines applicable to a whole country meaning guidelines from countries with differing healthcare systems within the country may have been excluded.
Conclusions: National guidelines for dementia vary in their consideration of protected characteristics. We found that around a fifth of the world's countries have guidelines for dementia. We have identified areas of good practice that can be considered for future guidelines and suggest that all guidelines provide specific evidence-based recommendations for minority groups with examples of how to implement them. This will promote equity in the care of people affected by dementia and help to ensure that people with protected characteristics also have high-quality clinical services.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


