Caroline McCarthy, Barbara Clyne, Fiona Boland, Frank Moriarty, Michelle Flood, Emma Wallace, Susan M Smith
{"title":"由全科医生对爱尔兰基层医疗机构中身患多种疾病的老年人的多药治疗、取消处方和患者优先权进行药物审查(SPPiRE 研究):分组随机对照试验。","authors":"Caroline McCarthy, Barbara Clyne, Fiona Boland, Frank Moriarty, Michelle Flood, Emma Wallace, Susan M Smith","doi":"10.1371/journal.pmed.1003862","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a rising prevalence of multimorbidity, particularly in older patients, and a need for evidence-based medicines management interventions for this population. The Supporting Prescribing in Older Adults with Multimorbidity in Irish Primary Care (SPPiRE) trial aimed to investigate the effect of a general practitioner (GP)-delivered, individualised medication review in reducing polypharmacy and potentially inappropriate prescriptions (PIPs) in community-dwelling older patients with multimorbidity in primary care.</p><p><strong>Methods and findings: </strong>We conducted a cluster randomised controlled trial (RCT) set in 51 GP practices throughout the Republic of Ireland. A total of 404 patients, aged ≥65 years with complex multimorbidity, defined as being prescribed ≥15 regular medicines, were recruited from April 2017 and followed up until October 2020. Furthermore, 26 intervention GP practices received access to the SPPiRE website where they completed an educational module and used a template for an individualised patient medication review that identified PIP, opportunities for deprescribing, and patient priorities for care. A total of 25 control GP practices delivered usual care. An independent blinded pharmacist assessed primary outcome measures that were the number of medicines and the proportion of patients with any PIP (from a predefined list of 34 indicators based predominantly on the STOPP/START version 2 criteria). We performed an intention-to-treat analysis using multilevel modelling. Recruited participants had substantial disease and treatment burden at baseline with a mean of 17.37 (standard deviation [SD] 3.50) medicines. At 6-month follow-up, both intervention and control groups had reductions in the numbers of medicines with a small but significantly greater reduction in the intervention group (incidence rate ratio [IRR] 0.95, 95% confidence interval [CI]: 0.899 to 0.999, p = 0.045). There was no significant effect on the odds of having at least 1 PIP in the intervention versus control group (odds ratio [OR] 0.39, 95% CI: 0.140 to 1.064, p = 0.066). Adverse events recorded included mortality, emergency department (ED) presentations, and adverse drug withdrawal events (ADWEs), and there was no evidence of harm. Less than 2% of drug withdrawals in the intervention group led to a reported ADWE. Due to the inability to electronically extract data, primary outcomes were measured at just 2 time points, and this is the main limitation of this work.</p><p><strong>Conclusions: </strong>The SPPiRE intervention resulted in a small but significant reduction in the number of medicines but no evidence of a clear effect on PIP. This reduction in significant polypharmacy may have more of an impact at a population rather than individual patient level.</p><p><strong>Trial registration: </strong>ISRCTN Registry ISRCTN12752680.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 1","pages":"e1003862"},"PeriodicalIF":9.9000,"publicationDate":"2022-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8730438/pdf/","citationCount":"0","resultStr":"{\"title\":\"GP-delivered medication review of polypharmacy, deprescribing, and patient priorities in older people with multimorbidity in Irish primary care (SPPiRE Study): A cluster randomised controlled trial.\",\"authors\":\"Caroline McCarthy, Barbara Clyne, Fiona Boland, Frank Moriarty, Michelle Flood, Emma Wallace, Susan M Smith\",\"doi\":\"10.1371/journal.pmed.1003862\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is a rising prevalence of multimorbidity, particularly in older patients, and a need for evidence-based medicines management interventions for this population. The Supporting Prescribing in Older Adults with Multimorbidity in Irish Primary Care (SPPiRE) trial aimed to investigate the effect of a general practitioner (GP)-delivered, individualised medication review in reducing polypharmacy and potentially inappropriate prescriptions (PIPs) in community-dwelling older patients with multimorbidity in primary care.</p><p><strong>Methods and findings: </strong>We conducted a cluster randomised controlled trial (RCT) set in 51 GP practices throughout the Republic of Ireland. A total of 404 patients, aged ≥65 years with complex multimorbidity, defined as being prescribed ≥15 regular medicines, were recruited from April 2017 and followed up until October 2020. Furthermore, 26 intervention GP practices received access to the SPPiRE website where they completed an educational module and used a template for an individualised patient medication review that identified PIP, opportunities for deprescribing, and patient priorities for care. A total of 25 control GP practices delivered usual care. An independent blinded pharmacist assessed primary outcome measures that were the number of medicines and the proportion of patients with any PIP (from a predefined list of 34 indicators based predominantly on the STOPP/START version 2 criteria). We performed an intention-to-treat analysis using multilevel modelling. Recruited participants had substantial disease and treatment burden at baseline with a mean of 17.37 (standard deviation [SD] 3.50) medicines. At 6-month follow-up, both intervention and control groups had reductions in the numbers of medicines with a small but significantly greater reduction in the intervention group (incidence rate ratio [IRR] 0.95, 95% confidence interval [CI]: 0.899 to 0.999, p = 0.045). There was no significant effect on the odds of having at least 1 PIP in the intervention versus control group (odds ratio [OR] 0.39, 95% CI: 0.140 to 1.064, p = 0.066). Adverse events recorded included mortality, emergency department (ED) presentations, and adverse drug withdrawal events (ADWEs), and there was no evidence of harm. Less than 2% of drug withdrawals in the intervention group led to a reported ADWE. Due to the inability to electronically extract data, primary outcomes were measured at just 2 time points, and this is the main limitation of this work.</p><p><strong>Conclusions: </strong>The SPPiRE intervention resulted in a small but significant reduction in the number of medicines but no evidence of a clear effect on PIP. This reduction in significant polypharmacy may have more of an impact at a population rather than individual patient level.</p><p><strong>Trial registration: </strong>ISRCTN Registry ISRCTN12752680.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 1\",\"pages\":\"e1003862\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2022-01-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8730438/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003862\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003862","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
GP-delivered medication review of polypharmacy, deprescribing, and patient priorities in older people with multimorbidity in Irish primary care (SPPiRE Study): A cluster randomised controlled trial.
Background: There is a rising prevalence of multimorbidity, particularly in older patients, and a need for evidence-based medicines management interventions for this population. The Supporting Prescribing in Older Adults with Multimorbidity in Irish Primary Care (SPPiRE) trial aimed to investigate the effect of a general practitioner (GP)-delivered, individualised medication review in reducing polypharmacy and potentially inappropriate prescriptions (PIPs) in community-dwelling older patients with multimorbidity in primary care.
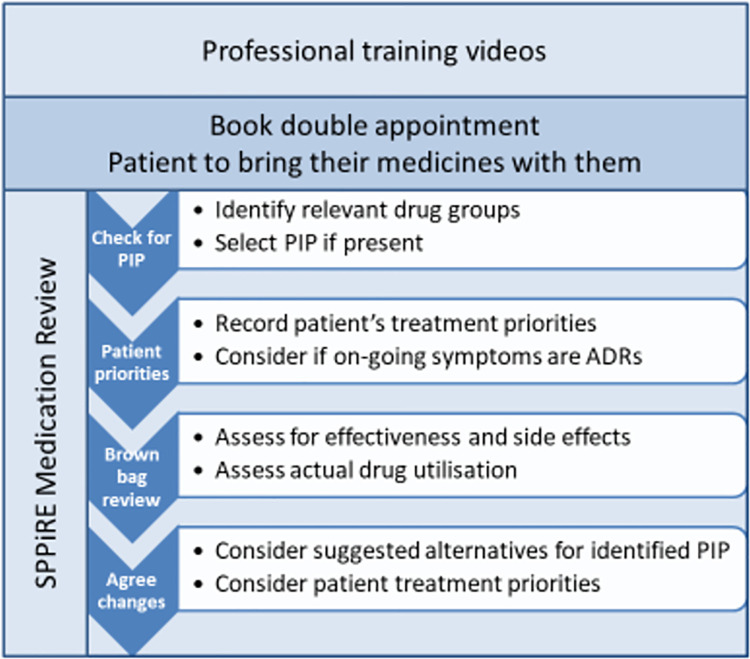
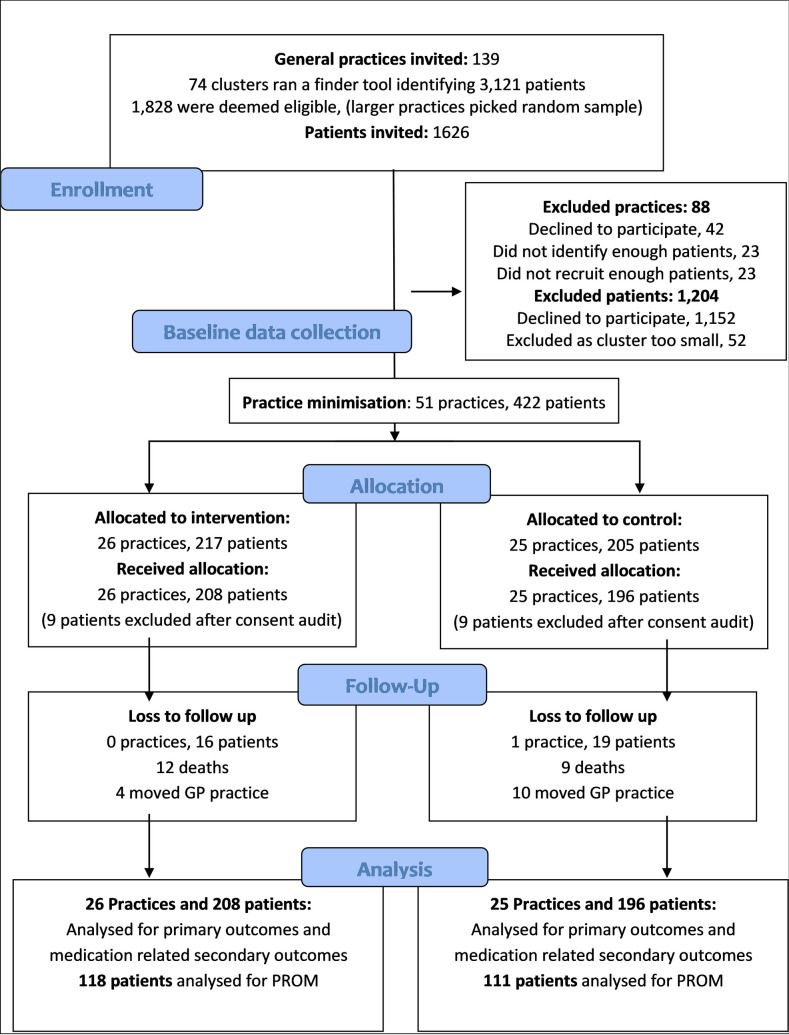
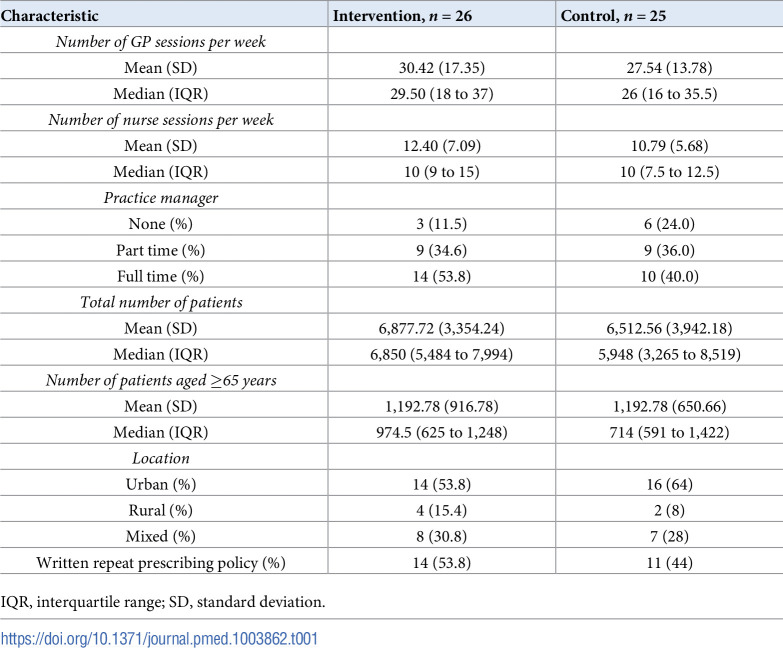
Methods and findings: We conducted a cluster randomised controlled trial (RCT) set in 51 GP practices throughout the Republic of Ireland. A total of 404 patients, aged ≥65 years with complex multimorbidity, defined as being prescribed ≥15 regular medicines, were recruited from April 2017 and followed up until October 2020. Furthermore, 26 intervention GP practices received access to the SPPiRE website where they completed an educational module and used a template for an individualised patient medication review that identified PIP, opportunities for deprescribing, and patient priorities for care. A total of 25 control GP practices delivered usual care. An independent blinded pharmacist assessed primary outcome measures that were the number of medicines and the proportion of patients with any PIP (from a predefined list of 34 indicators based predominantly on the STOPP/START version 2 criteria). We performed an intention-to-treat analysis using multilevel modelling. Recruited participants had substantial disease and treatment burden at baseline with a mean of 17.37 (standard deviation [SD] 3.50) medicines. At 6-month follow-up, both intervention and control groups had reductions in the numbers of medicines with a small but significantly greater reduction in the intervention group (incidence rate ratio [IRR] 0.95, 95% confidence interval [CI]: 0.899 to 0.999, p = 0.045). There was no significant effect on the odds of having at least 1 PIP in the intervention versus control group (odds ratio [OR] 0.39, 95% CI: 0.140 to 1.064, p = 0.066). Adverse events recorded included mortality, emergency department (ED) presentations, and adverse drug withdrawal events (ADWEs), and there was no evidence of harm. Less than 2% of drug withdrawals in the intervention group led to a reported ADWE. Due to the inability to electronically extract data, primary outcomes were measured at just 2 time points, and this is the main limitation of this work.
Conclusions: The SPPiRE intervention resulted in a small but significant reduction in the number of medicines but no evidence of a clear effect on PIP. This reduction in significant polypharmacy may have more of an impact at a population rather than individual patient level.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


