{"title":"CD3/CD19去除t细胞减少的异体移植:大部分是有效的,但不是稳健的。","authors":"Eliza Wiercinska, Erhard Seifried, Halvard Bonig","doi":"10.2991/chi.k.210725.001","DOIUrl":null,"url":null,"abstract":"<p><p>Aggressive T-cell depletion, <i>in vitro</i> or <i>in vivo</i>, is a prerequisite for survival of haplo-identical stem cell transplantation. The classical T-cell-depleted transplant, immunomagnetically enriched CD34+ cells, is very safe with respect to graft-versus-host reactivity, but associated with very high transplant-related and relapse mortality with an overall probability of survival of only 20%. Protocols for T- and B-cell depletion were therefore developed, reasoning that transplantation of the majority of Natural Killer (NK) cells and the substantial dose of residual T-cells might improve survival, which was, in principle, confirmed. Anecdotal reports of frequent failure to achieve adequate T-cell depletion prompted review of the aggregate data for transplant quality at our center. The first observation is the relative paucity of combined CD3/CD19 depletion processes as PTCy protocols have made inroads, 13 depletions in 8 years. Median T- and B-cell log-depletion were -3.89 and -1.92, respectively; instead of, CD34+ cell recovery was generally high (median 92%), as was NK-cell recovery (median 52%). However, the process failed to yield satisfactory T- and B-cell depletion in two out of 13 preparations, of which one product could be rescued by a second round of depletion, at the expense of CD34+ cell recovery. In our hands, the process is thus insufficiently robust for routine clinical use. Assuming similar observations in other centers, this may explain implementation of alternative protocols, such as TCR<i>αβ</i>/CD19 depletion or transplantation of unmanipulated grafts with subsequent <i>in vivo</i> depletion.</p>","PeriodicalId":10368,"journal":{"name":"Clinical Hematology International","volume":"3 3","pages":"103-107"},"PeriodicalIF":0.0000,"publicationDate":"2021-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/f3/CHI-3-3-103.PMC8486974.pdf","citationCount":"3","resultStr":"{\"title\":\"CD3/CD19 Depletion for T-cell Reduction of Allogeneic Transplants: Mostly Efficient, but not Robust.\",\"authors\":\"Eliza Wiercinska, Erhard Seifried, Halvard Bonig\",\"doi\":\"10.2991/chi.k.210725.001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Aggressive T-cell depletion, <i>in vitro</i> or <i>in vivo</i>, is a prerequisite for survival of haplo-identical stem cell transplantation. The classical T-cell-depleted transplant, immunomagnetically enriched CD34+ cells, is very safe with respect to graft-versus-host reactivity, but associated with very high transplant-related and relapse mortality with an overall probability of survival of only 20%. Protocols for T- and B-cell depletion were therefore developed, reasoning that transplantation of the majority of Natural Killer (NK) cells and the substantial dose of residual T-cells might improve survival, which was, in principle, confirmed. Anecdotal reports of frequent failure to achieve adequate T-cell depletion prompted review of the aggregate data for transplant quality at our center. The first observation is the relative paucity of combined CD3/CD19 depletion processes as PTCy protocols have made inroads, 13 depletions in 8 years. Median T- and B-cell log-depletion were -3.89 and -1.92, respectively; instead of, CD34+ cell recovery was generally high (median 92%), as was NK-cell recovery (median 52%). However, the process failed to yield satisfactory T- and B-cell depletion in two out of 13 preparations, of which one product could be rescued by a second round of depletion, at the expense of CD34+ cell recovery. In our hands, the process is thus insufficiently robust for routine clinical use. Assuming similar observations in other centers, this may explain implementation of alternative protocols, such as TCR<i>αβ</i>/CD19 depletion or transplantation of unmanipulated grafts with subsequent <i>in vivo</i> depletion.</p>\",\"PeriodicalId\":10368,\"journal\":{\"name\":\"Clinical Hematology International\",\"volume\":\"3 3\",\"pages\":\"103-107\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/f3/CHI-3-3-103.PMC8486974.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Hematology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2991/chi.k.210725.001\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hematology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2991/chi.k.210725.001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
CD3/CD19 Depletion for T-cell Reduction of Allogeneic Transplants: Mostly Efficient, but not Robust.
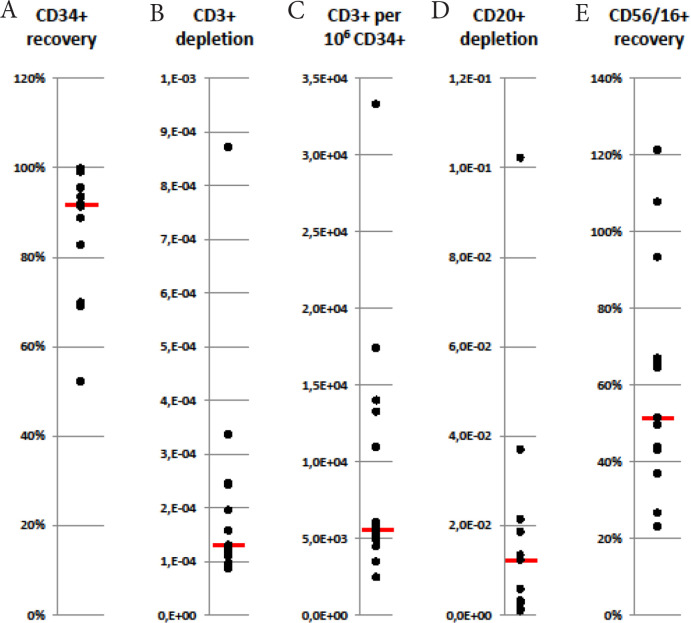
Aggressive T-cell depletion, in vitro or in vivo, is a prerequisite for survival of haplo-identical stem cell transplantation. The classical T-cell-depleted transplant, immunomagnetically enriched CD34+ cells, is very safe with respect to graft-versus-host reactivity, but associated with very high transplant-related and relapse mortality with an overall probability of survival of only 20%. Protocols for T- and B-cell depletion were therefore developed, reasoning that transplantation of the majority of Natural Killer (NK) cells and the substantial dose of residual T-cells might improve survival, which was, in principle, confirmed. Anecdotal reports of frequent failure to achieve adequate T-cell depletion prompted review of the aggregate data for transplant quality at our center. The first observation is the relative paucity of combined CD3/CD19 depletion processes as PTCy protocols have made inroads, 13 depletions in 8 years. Median T- and B-cell log-depletion were -3.89 and -1.92, respectively; instead of, CD34+ cell recovery was generally high (median 92%), as was NK-cell recovery (median 52%). However, the process failed to yield satisfactory T- and B-cell depletion in two out of 13 preparations, of which one product could be rescued by a second round of depletion, at the expense of CD34+ cell recovery. In our hands, the process is thus insufficiently robust for routine clinical use. Assuming similar observations in other centers, this may explain implementation of alternative protocols, such as TCRαβ/CD19 depletion or transplantation of unmanipulated grafts with subsequent in vivo depletion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


