Julia L Jones, Natalie G Lumsden, Koen Simons, Anis Ta'eed, Maximilian P de Courten, Tissa Wijeratne, Nicholas Cox, Christopher J A Neil, Jo-Anne Manski-Nankervis, Peter Shane Hamblin, Edward D Janus, Craig L Nelson
{"title":"使用电子病历数据评估慢性肾脏疾病、2型糖尿病和心血管疾病的检测、识别和管理,记录在澳大利亚的一般做法:横断面分析。","authors":"Julia L Jones, Natalie G Lumsden, Koen Simons, Anis Ta'eed, Maximilian P de Courten, Tissa Wijeratne, Nicholas Cox, Christopher J A Neil, Jo-Anne Manski-Nankervis, Peter Shane Hamblin, Edward D Janus, Craig L Nelson","doi":"10.1136/fmch-2021-001006","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the capacity of general practice (GP) electronic medical record (EMR) data to assess risk factor detection, disease diagnostic testing, diagnosis, monitoring and pharmacotherapy for the interrelated chronic vascular diseases-chronic kidney disease (CKD), type 2 diabetes (T2D) and cardiovascular disease.</p><p><strong>Design: </strong>Cross-sectional analysis of data extracted on a single date for each practice between 12 April 2017 and 18 April 2017 incorporating data from any time on or before data extraction, using baseline data from the Chronic Disease early detection and Improved Management in PrimAry Care ProjecT. Deidentified data were extracted from GP EMRs using the Pen Computer Systems Clinical Audit Tool and descriptive statistics used to describe the study population.</p><p><strong>Setting: </strong>Eight GPs in Victoria, Australia.</p><p><strong>Participants: </strong>Patients were ≥18 years and attended GP ≥3 times within 24 months. 37 946 patients were included.</p><p><strong>Results: </strong>Risk factor and disease testing/monitoring/treatment were assessed as per Australian guidelines (or US guidelines if none available), with guidelines simplified due to limitations in data availability where required. Risk factor assessment in those requiring it: 30% of patients had body mass index and 46% blood pressure within guideline recommended timeframes. Diagnostic testing in at-risk population: 17% had diagnostic testing as per recommendations for CKD and 37% for T2D. Possible undiagnosed disease: Pathology tests indicating possible disease with no diagnosis already coded were present in 6.7% for CKD, 1.6% for T2D and 0.33% familial hypercholesterolaemia. Overall prevalence: Coded diagnoses were recorded in 3.8% for CKD, 6.6% for T2D, 4.2% for ischaemic heart disease, 1% for heart failure, 1.7% for ischaemic stroke, 0.46% for peripheral vascular disease, 0.06% for familial hypercholesterolaemia and 2% for atrial fibrillation. Pharmaceutical prescriptions: the proportion of patients prescribed guideline-recommended medications ranged from 44% (beta blockers for patients with ischaemic heart disease) to 78% (antiplatelets or anticoagulants for patients with ischaemic stroke).</p><p><strong>Conclusions: </strong>Using GP EMR data, this study identified recorded diagnoses of chronic vascular diseases generally similar to, or higher than, reported national prevalence. It suggested low levels of extractable documented risk factor assessments, diagnostic testing in those at risk and prescription of guideline-recommended pharmacotherapy for some conditions. These baseline data highlight the utility of GP EMR data for potential use in epidemiological studies and by individual practices to guide targeted quality improvement. It also highlighted some of the challenges of using GP EMR data.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"10 1","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2022-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/eb/59/fmch-2021-001006.PMC8860071.pdf","citationCount":"2","resultStr":"{\"title\":\"Using electronic medical record data to assess chronic kidney disease, type 2 diabetes and cardiovascular disease testing, recognition and management as documented in Australian general practice: a cross-sectional analysis.\",\"authors\":\"Julia L Jones, Natalie G Lumsden, Koen Simons, Anis Ta'eed, Maximilian P de Courten, Tissa Wijeratne, Nicholas Cox, Christopher J A Neil, Jo-Anne Manski-Nankervis, Peter Shane Hamblin, Edward D Janus, Craig L Nelson\",\"doi\":\"10.1136/fmch-2021-001006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the capacity of general practice (GP) electronic medical record (EMR) data to assess risk factor detection, disease diagnostic testing, diagnosis, monitoring and pharmacotherapy for the interrelated chronic vascular diseases-chronic kidney disease (CKD), type 2 diabetes (T2D) and cardiovascular disease.</p><p><strong>Design: </strong>Cross-sectional analysis of data extracted on a single date for each practice between 12 April 2017 and 18 April 2017 incorporating data from any time on or before data extraction, using baseline data from the Chronic Disease early detection and Improved Management in PrimAry Care ProjecT. Deidentified data were extracted from GP EMRs using the Pen Computer Systems Clinical Audit Tool and descriptive statistics used to describe the study population.</p><p><strong>Setting: </strong>Eight GPs in Victoria, Australia.</p><p><strong>Participants: </strong>Patients were ≥18 years and attended GP ≥3 times within 24 months. 37 946 patients were included.</p><p><strong>Results: </strong>Risk factor and disease testing/monitoring/treatment were assessed as per Australian guidelines (or US guidelines if none available), with guidelines simplified due to limitations in data availability where required. Risk factor assessment in those requiring it: 30% of patients had body mass index and 46% blood pressure within guideline recommended timeframes. Diagnostic testing in at-risk population: 17% had diagnostic testing as per recommendations for CKD and 37% for T2D. Possible undiagnosed disease: Pathology tests indicating possible disease with no diagnosis already coded were present in 6.7% for CKD, 1.6% for T2D and 0.33% familial hypercholesterolaemia. Overall prevalence: Coded diagnoses were recorded in 3.8% for CKD, 6.6% for T2D, 4.2% for ischaemic heart disease, 1% for heart failure, 1.7% for ischaemic stroke, 0.46% for peripheral vascular disease, 0.06% for familial hypercholesterolaemia and 2% for atrial fibrillation. Pharmaceutical prescriptions: the proportion of patients prescribed guideline-recommended medications ranged from 44% (beta blockers for patients with ischaemic heart disease) to 78% (antiplatelets or anticoagulants for patients with ischaemic stroke).</p><p><strong>Conclusions: </strong>Using GP EMR data, this study identified recorded diagnoses of chronic vascular diseases generally similar to, or higher than, reported national prevalence. It suggested low levels of extractable documented risk factor assessments, diagnostic testing in those at risk and prescription of guideline-recommended pharmacotherapy for some conditions. These baseline data highlight the utility of GP EMR data for potential use in epidemiological studies and by individual practices to guide targeted quality improvement. It also highlighted some of the challenges of using GP EMR data.</p>\",\"PeriodicalId\":44590,\"journal\":{\"name\":\"Family Medicine and Community Health\",\"volume\":\"10 1\",\"pages\":\"\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2022-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/eb/59/fmch-2021-001006.PMC8860071.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Family Medicine and Community Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/fmch-2021-001006\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2021-001006","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Using electronic medical record data to assess chronic kidney disease, type 2 diabetes and cardiovascular disease testing, recognition and management as documented in Australian general practice: a cross-sectional analysis.
Objectives: To evaluate the capacity of general practice (GP) electronic medical record (EMR) data to assess risk factor detection, disease diagnostic testing, diagnosis, monitoring and pharmacotherapy for the interrelated chronic vascular diseases-chronic kidney disease (CKD), type 2 diabetes (T2D) and cardiovascular disease.
Design: Cross-sectional analysis of data extracted on a single date for each practice between 12 April 2017 and 18 April 2017 incorporating data from any time on or before data extraction, using baseline data from the Chronic Disease early detection and Improved Management in PrimAry Care ProjecT. Deidentified data were extracted from GP EMRs using the Pen Computer Systems Clinical Audit Tool and descriptive statistics used to describe the study population.
Setting: Eight GPs in Victoria, Australia.
Participants: Patients were ≥18 years and attended GP ≥3 times within 24 months. 37 946 patients were included.
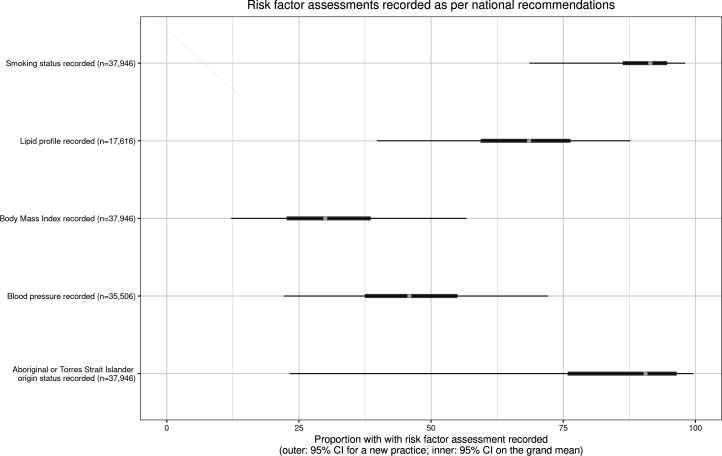
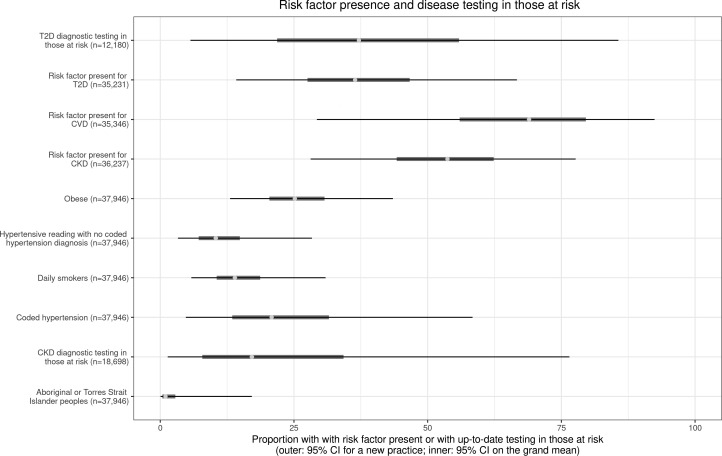
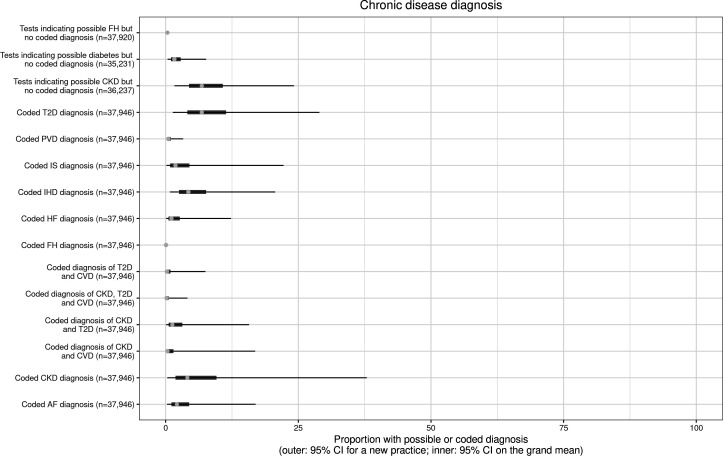
Results: Risk factor and disease testing/monitoring/treatment were assessed as per Australian guidelines (or US guidelines if none available), with guidelines simplified due to limitations in data availability where required. Risk factor assessment in those requiring it: 30% of patients had body mass index and 46% blood pressure within guideline recommended timeframes. Diagnostic testing in at-risk population: 17% had diagnostic testing as per recommendations for CKD and 37% for T2D. Possible undiagnosed disease: Pathology tests indicating possible disease with no diagnosis already coded were present in 6.7% for CKD, 1.6% for T2D and 0.33% familial hypercholesterolaemia. Overall prevalence: Coded diagnoses were recorded in 3.8% for CKD, 6.6% for T2D, 4.2% for ischaemic heart disease, 1% for heart failure, 1.7% for ischaemic stroke, 0.46% for peripheral vascular disease, 0.06% for familial hypercholesterolaemia and 2% for atrial fibrillation. Pharmaceutical prescriptions: the proportion of patients prescribed guideline-recommended medications ranged from 44% (beta blockers for patients with ischaemic heart disease) to 78% (antiplatelets or anticoagulants for patients with ischaemic stroke).
Conclusions: Using GP EMR data, this study identified recorded diagnoses of chronic vascular diseases generally similar to, or higher than, reported national prevalence. It suggested low levels of extractable documented risk factor assessments, diagnostic testing in those at risk and prescription of guideline-recommended pharmacotherapy for some conditions. These baseline data highlight the utility of GP EMR data for potential use in epidemiological studies and by individual practices to guide targeted quality improvement. It also highlighted some of the challenges of using GP EMR data.
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


