Samuel S Bruce, Babak B Navi, Cenai Zhang, Jiwon Kim, Richard B Devereux, Edward J Schenck, Art Sedrakyan, Iván Díaz, Hooman Kamel
{"title":"经食管超声心动图与缺血性卒中或短暂性缺血性发作患者呼吸衰竭的风险:一项IDEAL 4期研究","authors":"Samuel S Bruce, Babak B Navi, Cenai Zhang, Jiwon Kim, Richard B Devereux, Edward J Schenck, Art Sedrakyan, Iván Díaz, Hooman Kamel","doi":"10.1136/bmjsit-2021-000116","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Transesophageal echocardiography (TEE) is sometimes used to search for cardioembolic sources after ischemic stroke or transient ischemic attack (TIA). TEE visualizes some sources better than transthoracic echocardiography, but TEE is invasive and may cause aspiration. Few data exist on the risk of respiratory complications after TEE in patients who had stroke or TIA. Our objective was to determine whether TEE was associated with increased risk of respiratory failure in patients who had ischemic stroke or TIA.</p><p><strong>Design: </strong>This is a retrospective cohort study using administrative data from inpatient and outpatient insurance claims collected by the US federal government's Centers for Medicare and Medicaid Services.</p><p><strong>Setting: </strong>Hospitals and outpatient clinics throughout the USA.</p><p><strong>Participants: </strong>99 081 patients ≥65 years old hospitalized for out-of-hospital ischemic stroke or TIA, defined by validated International Classification of Disease-9/10 diagnosis codes and present-on-admission codes, using claims data from 2008 to 2018 in a random 5% sample of Medicare beneficiaries.</p><p><strong>Main outcome measures: </strong>Acute respiratory failure, defined as endotracheal intubation and/or mechanical ventilation, starting on the first day after admission through 28 days afterward.</p><p><strong>Results: </strong>Of 99 081 patients included in this analysis, 73 733 (74.4%) had an ischemic stroke and 25 348 (25.6%) a TIA. TEE was performed in 4677 (4.7%) patients and intubation and/or mechanical ventilation in 1403 (1.4%) patients. The 28-day cumulative risk of respiratory failure after TEE (1.4%; 95% CI 0.8% to 2.7%) was similar to that seen in those without TEE (1.4%; 95% CI 1.4% to 1.5%) (p=0.84). After adjustment for age, sex, race, Charlson comorbidities, diagnosis of stroke versus TIA, intravenous thrombolysis, and mechanical thrombectomy, TEE was not associated with an increased risk of respiratory failure (HR, 0.9; 95% CI 0.6 to 1.2).</p><p><strong>Conclusions: </strong>In a cohort of older patients who had ischemic stroke or TIA, TEE was not associated with an increased risk of subsequent respiratory failure.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":" ","pages":"e000116"},"PeriodicalIF":1.6000,"publicationDate":"2022-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/18/bmjsit-2021-000116.PMC8823208.pdf","citationCount":"3","resultStr":"{\"title\":\"Transesophageal echocardiography and risk of respiratory failure in patients who had ischemic stroke or transient ischemic attack: an IDEAL phase 4 study.\",\"authors\":\"Samuel S Bruce, Babak B Navi, Cenai Zhang, Jiwon Kim, Richard B Devereux, Edward J Schenck, Art Sedrakyan, Iván Díaz, Hooman Kamel\",\"doi\":\"10.1136/bmjsit-2021-000116\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Transesophageal echocardiography (TEE) is sometimes used to search for cardioembolic sources after ischemic stroke or transient ischemic attack (TIA). TEE visualizes some sources better than transthoracic echocardiography, but TEE is invasive and may cause aspiration. Few data exist on the risk of respiratory complications after TEE in patients who had stroke or TIA. Our objective was to determine whether TEE was associated with increased risk of respiratory failure in patients who had ischemic stroke or TIA.</p><p><strong>Design: </strong>This is a retrospective cohort study using administrative data from inpatient and outpatient insurance claims collected by the US federal government's Centers for Medicare and Medicaid Services.</p><p><strong>Setting: </strong>Hospitals and outpatient clinics throughout the USA.</p><p><strong>Participants: </strong>99 081 patients ≥65 years old hospitalized for out-of-hospital ischemic stroke or TIA, defined by validated International Classification of Disease-9/10 diagnosis codes and present-on-admission codes, using claims data from 2008 to 2018 in a random 5% sample of Medicare beneficiaries.</p><p><strong>Main outcome measures: </strong>Acute respiratory failure, defined as endotracheal intubation and/or mechanical ventilation, starting on the first day after admission through 28 days afterward.</p><p><strong>Results: </strong>Of 99 081 patients included in this analysis, 73 733 (74.4%) had an ischemic stroke and 25 348 (25.6%) a TIA. TEE was performed in 4677 (4.7%) patients and intubation and/or mechanical ventilation in 1403 (1.4%) patients. The 28-day cumulative risk of respiratory failure after TEE (1.4%; 95% CI 0.8% to 2.7%) was similar to that seen in those without TEE (1.4%; 95% CI 1.4% to 1.5%) (p=0.84). After adjustment for age, sex, race, Charlson comorbidities, diagnosis of stroke versus TIA, intravenous thrombolysis, and mechanical thrombectomy, TEE was not associated with an increased risk of respiratory failure (HR, 0.9; 95% CI 0.6 to 1.2).</p><p><strong>Conclusions: </strong>In a cohort of older patients who had ischemic stroke or TIA, TEE was not associated with an increased risk of subsequent respiratory failure.</p>\",\"PeriodicalId\":33349,\"journal\":{\"name\":\"BMJ Surgery Interventions Health Technologies\",\"volume\":\" \",\"pages\":\"e000116\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2022-02-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/18/bmjsit-2021-000116.PMC8823208.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Surgery Interventions Health Technologies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjsit-2021-000116\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2021-000116","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 3
摘要
目的:经食管超声心动图(TEE)有时用于寻找缺血性卒中或短暂性脑缺血发作(TIA)后的心脏栓塞源。TEE比经胸超声心动图能更好地显示某些来源,但TEE是侵入性的,可能导致误吸。很少有关于卒中或TIA患者TEE后呼吸系统并发症风险的数据。我们的目的是确定TEE是否与缺血性卒中或TIA患者呼吸衰竭风险增加有关。设计:这是一项回顾性队列研究,使用美国联邦政府医疗保险和医疗补助服务中心收集的住院和门诊保险索赔的行政数据。地点:美国各地的医院和门诊诊所。参与者:99081例≥65岁院外缺血性卒中或TIA住院患者,由经过验证的国际疾病分类9/10诊断代码和入院时代码定义,使用2008年至2018年的索赔数据,随机抽取5%的医疗保险受益人样本。主要结局指标:急性呼吸衰竭,定义为气管插管和/或机械通气,从入院后第一天开始至28天后。结果:纳入本分析的99 081例患者中,73 733例(74.4%)发生缺血性卒中,25 348例(25.6%)发生TIA。4677例(4.7%)患者行TEE, 1403例(1.4%)患者行插管和/或机械通气。TEE术后28天累积呼吸衰竭风险(1.4%;95% CI 0.8% - 2.7%)与未TEE患者相似(1.4%;95% CI 1.4% ~ 1.5%) (p=0.84)。在调整了年龄、性别、种族、Charlson合并症、卒中与TIA的诊断、静脉溶栓和机械取栓等因素后,TEE与呼吸衰竭风险增加无关(HR, 0.9;95% CI 0.6 - 1.2)。结论:在缺血性卒中或TIA的老年患者队列中,TEE与随后的呼吸衰竭风险增加无关。
Transesophageal echocardiography and risk of respiratory failure in patients who had ischemic stroke or transient ischemic attack: an IDEAL phase 4 study.
Objective: Transesophageal echocardiography (TEE) is sometimes used to search for cardioembolic sources after ischemic stroke or transient ischemic attack (TIA). TEE visualizes some sources better than transthoracic echocardiography, but TEE is invasive and may cause aspiration. Few data exist on the risk of respiratory complications after TEE in patients who had stroke or TIA. Our objective was to determine whether TEE was associated with increased risk of respiratory failure in patients who had ischemic stroke or TIA.
Design: This is a retrospective cohort study using administrative data from inpatient and outpatient insurance claims collected by the US federal government's Centers for Medicare and Medicaid Services.
Setting: Hospitals and outpatient clinics throughout the USA.
Participants: 99 081 patients ≥65 years old hospitalized for out-of-hospital ischemic stroke or TIA, defined by validated International Classification of Disease-9/10 diagnosis codes and present-on-admission codes, using claims data from 2008 to 2018 in a random 5% sample of Medicare beneficiaries.
Main outcome measures: Acute respiratory failure, defined as endotracheal intubation and/or mechanical ventilation, starting on the first day after admission through 28 days afterward.
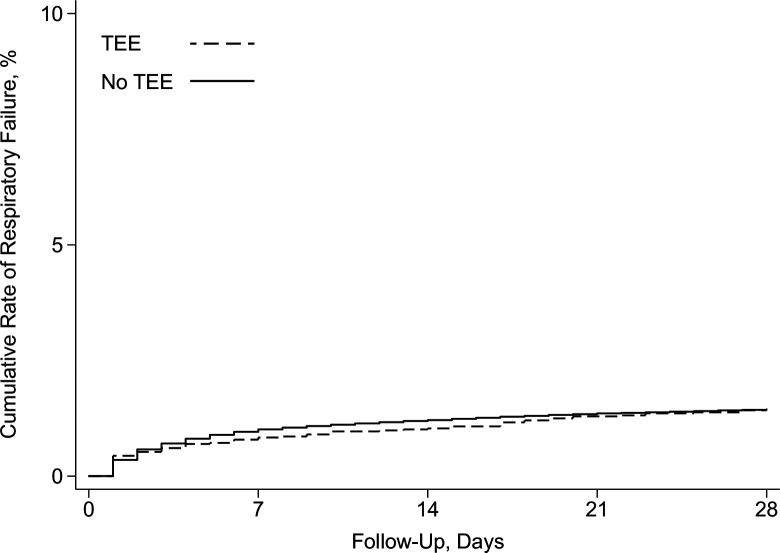
Results: Of 99 081 patients included in this analysis, 73 733 (74.4%) had an ischemic stroke and 25 348 (25.6%) a TIA. TEE was performed in 4677 (4.7%) patients and intubation and/or mechanical ventilation in 1403 (1.4%) patients. The 28-day cumulative risk of respiratory failure after TEE (1.4%; 95% CI 0.8% to 2.7%) was similar to that seen in those without TEE (1.4%; 95% CI 1.4% to 1.5%) (p=0.84). After adjustment for age, sex, race, Charlson comorbidities, diagnosis of stroke versus TIA, intravenous thrombolysis, and mechanical thrombectomy, TEE was not associated with an increased risk of respiratory failure (HR, 0.9; 95% CI 0.6 to 1.2).
Conclusions: In a cohort of older patients who had ischemic stroke or TIA, TEE was not associated with an increased risk of subsequent respiratory failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


