Patrick Russell, Udul Hewage, Cameron McDonald, Campbell Thompson, Richard Woodman, Arduino A Mangoni
{"title":"非特异性处方在老年住院病人出院到养老院的前瞻性队列研究。","authors":"Patrick Russell, Udul Hewage, Cameron McDonald, Campbell Thompson, Richard Woodman, Arduino A Mangoni","doi":"10.1177/20420986211052344","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Older patients from nursing homes are commonly exposed to polypharmacy before a hospital admission. Deprescribing has been promoted as a solution to this problem, though systematic reviews have not found benefit. The aim of this study was to understand if in-hospital deprescribing of certain classes of medications is associated with certain benefits or risks.</p><p><strong>Methods: </strong>We conducted a prospective, multicentre, cohort study in 239 medical inpatients ⩾75 years (mean age 87.4 years) who were exposed to polypharmacy (⩾5 medications) prior to admission and discharged to a nursing home for permanent placement. Patients were categorised by whether deprescribing occurred, mortality and readmissions were assessed 30 and 90 days after hospital discharge. The EQ-5D-5 L health survey assessed changes in health-related quality of life (HRQOL) at 90 days, with comparison to EQ-5D-5 L results at day 30. Latent class analysis (LCA) was used to investigate associations between patterns of prescribed and deprescribed medications and mortality.</p><p><strong>Results: </strong>Patients for whom deprescribing occurred had a higher Charlson Index; there were no differences between the groups in principal diagnosis, total or Beers list number of medications on admission. The number of Beers list medications increased in both groups before discharge. Patients who had medications deprescribed had nonsignificantly greater odds of dying within 90 days [odds ration (OR) = 3.23 (95% confidence interval (CI): 0.68, 14.92; p = 0.136]. Deprescribing of certain classes was associated with higher 90-day mortality: antihypertensives (OR = 2.27, 95% CI: 1.004, 5; <i>p</i> = 0.049) and statins (OR = 5, 95% CI: 1.61, 14.28; <i>p</i> = 0.005). Readmissions and 1-year mortality rates were similar. There was no deterioration in HRQOL when medications were deprescribed. LCA showed that patients with the least medication changes had the lowest mortality.</p><p><strong>Conclusion: </strong>Deprescribing certain classes of medications during hospitalisation was associated with worse mortality, but not readmissions or overall HRQOL. Larger controlled deprescribing studies targeting specific medications are warranted to further investigate these findings.This study was registered with the Australian and New Zealand Clinical Trials Registry, ACTRN1 2616001336471.</p><p><strong>Plain language summary: </strong><b>Background:</b> When an older person living in a nursing home is admitted to hospital, does stopping long-term medications help them?Many older people from nursing homes take a large number of medications each day to treat symptoms and prevent adverse events. \"Polypharmacy\" is a term used to describe taking multiple long-term medications, and it is associated with many negative outcomes such as increased number of falls, cognitive decline, hospital readmission, even death. Deprescribing of nonessential medications - whether stopping or reducing the dose - is promoted as good hospital practice and is assumed to help older frail people live longer and feel better. However, we often don't fully understand what is and is not essential.We wanted to better understand the effect of deprescribing long-term medications for older frail patients during an unplanned hospital admission as they were going to a nursing home to live.<b>Methods:</b> While admitted to hospital, medications are often reviewed by a clinical pharmacist and specialist physician. Sometimes medications are ceased; sometimes they are not. This gave us the opportunity to study two groups of older frail people from nursing homes: those who had regular, long-term medications ceased or reduced and those who did not. We wanted to see if one group did better. For example, did they feel worse if we stopped certain medications? Did they suffer other bad events compared with those patients for whom no medications were ceased? Were they readmitted to hospital earlier or more often?<b>Results and conclusion:</b> Despite the assumption that stopping medications for this type of patient is good practice, we found no benefit. We were also surprised to find stopping or reducing certain drug classes (e.g. antihypertensives and cholesterol-lowering drugs) was associated with greater mortality. Larger, randomised studies will better answer these important questions.</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":"12 ","pages":"20420986211052344"},"PeriodicalIF":3.4000,"publicationDate":"2021-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fd/eb/10.1177_20420986211052344.PMC8543714.pdf","citationCount":"4","resultStr":"{\"title\":\"Prospective cohort study of nonspecific deprescribing in older medical inpatients being discharged to a nursing home.\",\"authors\":\"Patrick Russell, Udul Hewage, Cameron McDonald, Campbell Thompson, Richard Woodman, Arduino A Mangoni\",\"doi\":\"10.1177/20420986211052344\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Older patients from nursing homes are commonly exposed to polypharmacy before a hospital admission. Deprescribing has been promoted as a solution to this problem, though systematic reviews have not found benefit. The aim of this study was to understand if in-hospital deprescribing of certain classes of medications is associated with certain benefits or risks.</p><p><strong>Methods: </strong>We conducted a prospective, multicentre, cohort study in 239 medical inpatients ⩾75 years (mean age 87.4 years) who were exposed to polypharmacy (⩾5 medications) prior to admission and discharged to a nursing home for permanent placement. Patients were categorised by whether deprescribing occurred, mortality and readmissions were assessed 30 and 90 days after hospital discharge. The EQ-5D-5 L health survey assessed changes in health-related quality of life (HRQOL) at 90 days, with comparison to EQ-5D-5 L results at day 30. Latent class analysis (LCA) was used to investigate associations between patterns of prescribed and deprescribed medications and mortality.</p><p><strong>Results: </strong>Patients for whom deprescribing occurred had a higher Charlson Index; there were no differences between the groups in principal diagnosis, total or Beers list number of medications on admission. The number of Beers list medications increased in both groups before discharge. Patients who had medications deprescribed had nonsignificantly greater odds of dying within 90 days [odds ration (OR) = 3.23 (95% confidence interval (CI): 0.68, 14.92; p = 0.136]. Deprescribing of certain classes was associated with higher 90-day mortality: antihypertensives (OR = 2.27, 95% CI: 1.004, 5; <i>p</i> = 0.049) and statins (OR = 5, 95% CI: 1.61, 14.28; <i>p</i> = 0.005). Readmissions and 1-year mortality rates were similar. There was no deterioration in HRQOL when medications were deprescribed. LCA showed that patients with the least medication changes had the lowest mortality.</p><p><strong>Conclusion: </strong>Deprescribing certain classes of medications during hospitalisation was associated with worse mortality, but not readmissions or overall HRQOL. Larger controlled deprescribing studies targeting specific medications are warranted to further investigate these findings.This study was registered with the Australian and New Zealand Clinical Trials Registry, ACTRN1 2616001336471.</p><p><strong>Plain language summary: </strong><b>Background:</b> When an older person living in a nursing home is admitted to hospital, does stopping long-term medications help them?Many older people from nursing homes take a large number of medications each day to treat symptoms and prevent adverse events. \\\"Polypharmacy\\\" is a term used to describe taking multiple long-term medications, and it is associated with many negative outcomes such as increased number of falls, cognitive decline, hospital readmission, even death. Deprescribing of nonessential medications - whether stopping or reducing the dose - is promoted as good hospital practice and is assumed to help older frail people live longer and feel better. However, we often don't fully understand what is and is not essential.We wanted to better understand the effect of deprescribing long-term medications for older frail patients during an unplanned hospital admission as they were going to a nursing home to live.<b>Methods:</b> While admitted to hospital, medications are often reviewed by a clinical pharmacist and specialist physician. Sometimes medications are ceased; sometimes they are not. This gave us the opportunity to study two groups of older frail people from nursing homes: those who had regular, long-term medications ceased or reduced and those who did not. We wanted to see if one group did better. For example, did they feel worse if we stopped certain medications? Did they suffer other bad events compared with those patients for whom no medications were ceased? Were they readmitted to hospital earlier or more often?<b>Results and conclusion:</b> Despite the assumption that stopping medications for this type of patient is good practice, we found no benefit. We were also surprised to find stopping or reducing certain drug classes (e.g. antihypertensives and cholesterol-lowering drugs) was associated with greater mortality. Larger, randomised studies will better answer these important questions.</p>\",\"PeriodicalId\":23012,\"journal\":{\"name\":\"Therapeutic Advances in Drug Safety\",\"volume\":\"12 \",\"pages\":\"20420986211052344\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2021-10-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fd/eb/10.1177_20420986211052344.PMC8543714.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20420986211052344\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986211052344","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Prospective cohort study of nonspecific deprescribing in older medical inpatients being discharged to a nursing home.
Background: Older patients from nursing homes are commonly exposed to polypharmacy before a hospital admission. Deprescribing has been promoted as a solution to this problem, though systematic reviews have not found benefit. The aim of this study was to understand if in-hospital deprescribing of certain classes of medications is associated with certain benefits or risks.
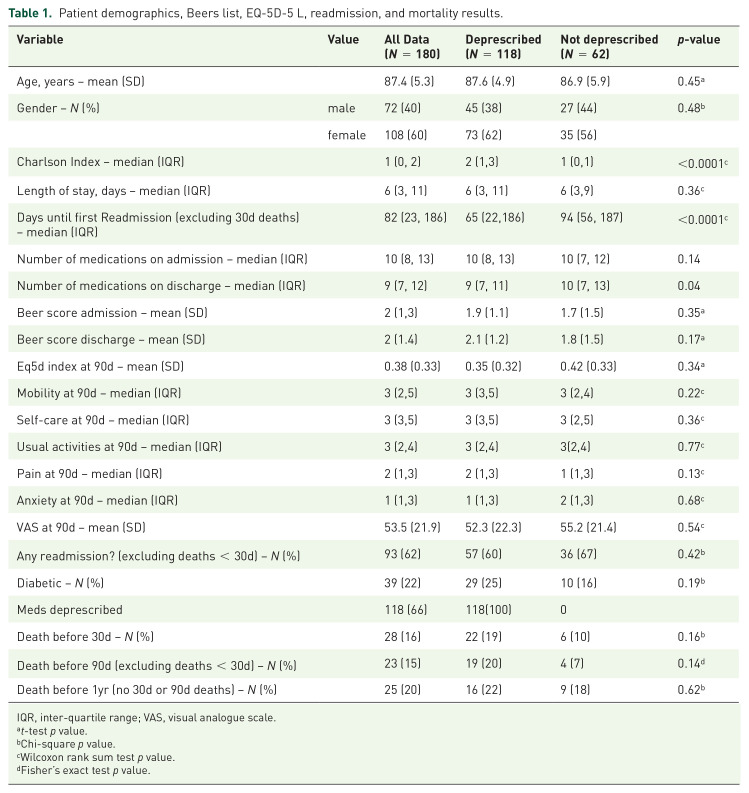
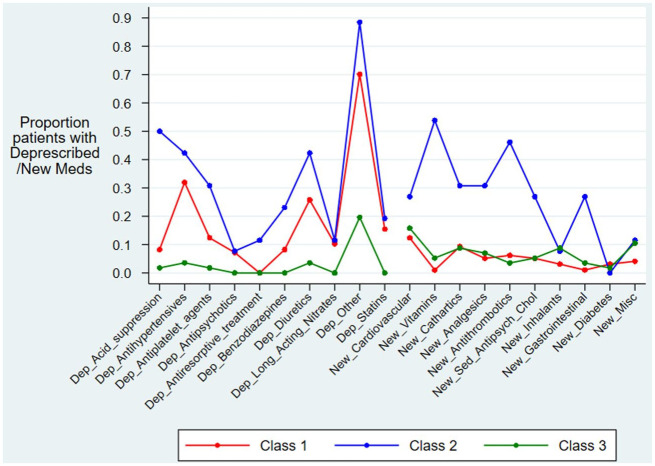
Methods: We conducted a prospective, multicentre, cohort study in 239 medical inpatients ⩾75 years (mean age 87.4 years) who were exposed to polypharmacy (⩾5 medications) prior to admission and discharged to a nursing home for permanent placement. Patients were categorised by whether deprescribing occurred, mortality and readmissions were assessed 30 and 90 days after hospital discharge. The EQ-5D-5 L health survey assessed changes in health-related quality of life (HRQOL) at 90 days, with comparison to EQ-5D-5 L results at day 30. Latent class analysis (LCA) was used to investigate associations between patterns of prescribed and deprescribed medications and mortality.
Results: Patients for whom deprescribing occurred had a higher Charlson Index; there were no differences between the groups in principal diagnosis, total or Beers list number of medications on admission. The number of Beers list medications increased in both groups before discharge. Patients who had medications deprescribed had nonsignificantly greater odds of dying within 90 days [odds ration (OR) = 3.23 (95% confidence interval (CI): 0.68, 14.92; p = 0.136]. Deprescribing of certain classes was associated with higher 90-day mortality: antihypertensives (OR = 2.27, 95% CI: 1.004, 5; p = 0.049) and statins (OR = 5, 95% CI: 1.61, 14.28; p = 0.005). Readmissions and 1-year mortality rates were similar. There was no deterioration in HRQOL when medications were deprescribed. LCA showed that patients with the least medication changes had the lowest mortality.
Conclusion: Deprescribing certain classes of medications during hospitalisation was associated with worse mortality, but not readmissions or overall HRQOL. Larger controlled deprescribing studies targeting specific medications are warranted to further investigate these findings.This study was registered with the Australian and New Zealand Clinical Trials Registry, ACTRN1 2616001336471.
Plain language summary: Background: When an older person living in a nursing home is admitted to hospital, does stopping long-term medications help them?Many older people from nursing homes take a large number of medications each day to treat symptoms and prevent adverse events. "Polypharmacy" is a term used to describe taking multiple long-term medications, and it is associated with many negative outcomes such as increased number of falls, cognitive decline, hospital readmission, even death. Deprescribing of nonessential medications - whether stopping or reducing the dose - is promoted as good hospital practice and is assumed to help older frail people live longer and feel better. However, we often don't fully understand what is and is not essential.We wanted to better understand the effect of deprescribing long-term medications for older frail patients during an unplanned hospital admission as they were going to a nursing home to live.Methods: While admitted to hospital, medications are often reviewed by a clinical pharmacist and specialist physician. Sometimes medications are ceased; sometimes they are not. This gave us the opportunity to study two groups of older frail people from nursing homes: those who had regular, long-term medications ceased or reduced and those who did not. We wanted to see if one group did better. For example, did they feel worse if we stopped certain medications? Did they suffer other bad events compared with those patients for whom no medications were ceased? Were they readmitted to hospital earlier or more often?Results and conclusion: Despite the assumption that stopping medications for this type of patient is good practice, we found no benefit. We were also surprised to find stopping or reducing certain drug classes (e.g. antihypertensives and cholesterol-lowering drugs) was associated with greater mortality. Larger, randomised studies will better answer these important questions.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


