Santhanalakshmi Gengiah, Catherine Connolly, Nonhlanhla Yende-Zuma, Pierre M Barker, Andrew J Nunn, Nesri Padayatchi, Myra Taylor, Marian Loveday, Kogieleum Naidoo
{"title":"预测质量改进协作方法成功的组织背景因素,以加强艾滋病毒/结核病综合服务:扩大结核病/艾滋病毒综合试验的子研究。","authors":"Santhanalakshmi Gengiah, Catherine Connolly, Nonhlanhla Yende-Zuma, Pierre M Barker, Andrew J Nunn, Nesri Padayatchi, Myra Taylor, Marian Loveday, Kogieleum Naidoo","doi":"10.1186/s13012-021-01155-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A quality improvement (QI) collaborative approach to enhancing integrated HIV-Tuberculosis (TB) services may be effective in scaling up and improving the quality of service delivery. Little is known of the role of organizational contextual factors (OCFs) in influencing the success of QI collaboratives. This study aims to determine which OCFs were associated with improvement in a QI collaborative intervention to enhance integrated HIV-TB services delivery.</p><p><strong>Methods: </strong>This is a nested sub-study embedded in a cluster-randomized controlled trial. Sixteen nurse supervisors (clusters) overseeing 40 clinics were randomized (1:1) to receive QI training and mentorship, or standard of care support (SOC). In the QI arm, eight nurse supervisors and 20 clinics formed a \"collaborative\" which aimed to improve HIV-TB process indicators, namely HIV testing, TB screening, isoniazid preventive therapy (IPT) initiations, viral load testing, and antiretroviral therapy for TB patients. OCFs measured at baseline were physical infrastructure, key staff, flexibility of clinic hours, monitoring data for improvement (MDI), and leadership support. Surveys were administered to clinic staff at baseline and month 12 to assess perceptions of supportiveness of contexts for change, and clinic organization for delivering integrated HIV-TB services. Linear mixed modelling was used to test for associations between OCFs and HIV-TB process indicators.</p><p><strong>Results: </strong>A total of 209 clinic staff participated in the study; 97 (46.4%) and 112 (53.6%) from QI and SOC arms, respectively. There were no differences between the QI and SOC arms scores achieved for physical infrastructure (78.9% vs 64.7%; p = 0.058), key staff (95.8 vs 92; p = 0.270), clinic hours (66.9 vs 65.5; p = 0.900), MDI (63.3 vs 65; p = 0.875, leadership support (46.0 vs 57.4; p = 0.265), and perceptions of supportiveness of contexts for change (76.2 vs 79.7; p = 0.128 and clinic organization for delivering integrated HIV-TB services (74.1 vs 80.1; p = 0.916). IPT initiation was the only indicator that was significantly improved in the parent study. MDI was a significantly associated with increasing IPT initiation rates [beta coefficient (β) = 0.004; p = 0.004].</p><p><strong>Discussion: </strong>MDI is a practice that should be fostered in public health facilities to increase the likelihood of success of future QI collaboratives to improve HIV-TB service delivery.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov , NCT02654613 . Registered 01 June 2015.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"88"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8447673/pdf/","citationCount":"0","resultStr":"{\"title\":\"Organizational contextual factors that predict success of a quality improvement collaborative approach to enhance integrated HIV-tuberculosis services: a sub-study of the Scaling up TB/HIV Integration trial.\",\"authors\":\"Santhanalakshmi Gengiah, Catherine Connolly, Nonhlanhla Yende-Zuma, Pierre M Barker, Andrew J Nunn, Nesri Padayatchi, Myra Taylor, Marian Loveday, Kogieleum Naidoo\",\"doi\":\"10.1186/s13012-021-01155-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A quality improvement (QI) collaborative approach to enhancing integrated HIV-Tuberculosis (TB) services may be effective in scaling up and improving the quality of service delivery. Little is known of the role of organizational contextual factors (OCFs) in influencing the success of QI collaboratives. This study aims to determine which OCFs were associated with improvement in a QI collaborative intervention to enhance integrated HIV-TB services delivery.</p><p><strong>Methods: </strong>This is a nested sub-study embedded in a cluster-randomized controlled trial. Sixteen nurse supervisors (clusters) overseeing 40 clinics were randomized (1:1) to receive QI training and mentorship, or standard of care support (SOC). In the QI arm, eight nurse supervisors and 20 clinics formed a \\\"collaborative\\\" which aimed to improve HIV-TB process indicators, namely HIV testing, TB screening, isoniazid preventive therapy (IPT) initiations, viral load testing, and antiretroviral therapy for TB patients. OCFs measured at baseline were physical infrastructure, key staff, flexibility of clinic hours, monitoring data for improvement (MDI), and leadership support. Surveys were administered to clinic staff at baseline and month 12 to assess perceptions of supportiveness of contexts for change, and clinic organization for delivering integrated HIV-TB services. Linear mixed modelling was used to test for associations between OCFs and HIV-TB process indicators.</p><p><strong>Results: </strong>A total of 209 clinic staff participated in the study; 97 (46.4%) and 112 (53.6%) from QI and SOC arms, respectively. There were no differences between the QI and SOC arms scores achieved for physical infrastructure (78.9% vs 64.7%; p = 0.058), key staff (95.8 vs 92; p = 0.270), clinic hours (66.9 vs 65.5; p = 0.900), MDI (63.3 vs 65; p = 0.875, leadership support (46.0 vs 57.4; p = 0.265), and perceptions of supportiveness of contexts for change (76.2 vs 79.7; p = 0.128 and clinic organization for delivering integrated HIV-TB services (74.1 vs 80.1; p = 0.916). IPT initiation was the only indicator that was significantly improved in the parent study. MDI was a significantly associated with increasing IPT initiation rates [beta coefficient (β) = 0.004; p = 0.004].</p><p><strong>Discussion: </strong>MDI is a practice that should be fostered in public health facilities to increase the likelihood of success of future QI collaboratives to improve HIV-TB service delivery.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov , NCT02654613 . Registered 01 June 2015.</p>\",\"PeriodicalId\":417097,\"journal\":{\"name\":\"Implementation Science : IS\",\"volume\":\" \",\"pages\":\"88\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-09-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8447673/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation Science : IS\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13012-021-01155-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13012-021-01155-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:采用质量改进(QI)协作方法来加强艾滋病毒-结核病(TB)综合服务可能有效地扩大和提高服务提供的质量。很少有人知道组织情境因素(ocf)在影响QI协作成功中的作用。本研究旨在确定哪些ocf与QI协作干预的改善有关,以加强艾滋病毒-结核病综合服务的提供。方法:这是一项嵌套的子研究,嵌入在一组随机对照试验中。监督40家诊所的16名护士主管(组)随机(1:1)接受QI培训和指导,或标准护理支持(SOC)。在QI部门,8名护士主管和20家诊所组成了一个“协作”,旨在改善艾滋病毒-结核病过程指标,即艾滋病毒检测、结核病筛查、异烟肼预防性治疗(IPT)启动、病毒载量检测和结核病患者抗逆转录病毒治疗。基线时测量的ocf包括物理基础设施、关键人员、门诊时间的灵活性、改善监测数据(MDI)和领导支持。在基线和第12个月对诊所工作人员进行调查,以评估对变革环境和诊所组织提供综合艾滋病毒-结核病服务的支持度的看法。线性混合模型用于测试ocf与HIV-TB过程指标之间的关联。结果:共有209名临床工作人员参与研究;QI组97例(46.4%),SOC组112例(53.6%)。物理基础设施的QI和SOC得分之间没有差异(78.9% vs 64.7%;P = 0.058),关键人员(95.8 vs 92;P = 0.270),就诊时间(66.9 vs 65.5;p = 0.900), MDI (63.3 vs 65;P = 0.875,领导支持度(46.0 vs 57.4;P = 0.265),以及对变化环境支持度的感知(76.2 vs 79.7;p = 0.128和提供艾滋病毒-结核病综合服务的诊所组织(74.1 vs 80.1;P = 0.916)。在父母研究中,IPT起始是唯一显著改善的指标。MDI与IPT起始率增加显著相关[β系数(β) = 0.004;P = 0.004]。讨论:MDI是一种应在公共卫生设施中加以促进的做法,以增加未来QI合作成功改善艾滋病毒-结核病服务提供的可能性。试验注册:Clinicaltrials.gov, NCT02654613。注册于2015年6月1日。
Organizational contextual factors that predict success of a quality improvement collaborative approach to enhance integrated HIV-tuberculosis services: a sub-study of the Scaling up TB/HIV Integration trial.
Background: A quality improvement (QI) collaborative approach to enhancing integrated HIV-Tuberculosis (TB) services may be effective in scaling up and improving the quality of service delivery. Little is known of the role of organizational contextual factors (OCFs) in influencing the success of QI collaboratives. This study aims to determine which OCFs were associated with improvement in a QI collaborative intervention to enhance integrated HIV-TB services delivery.
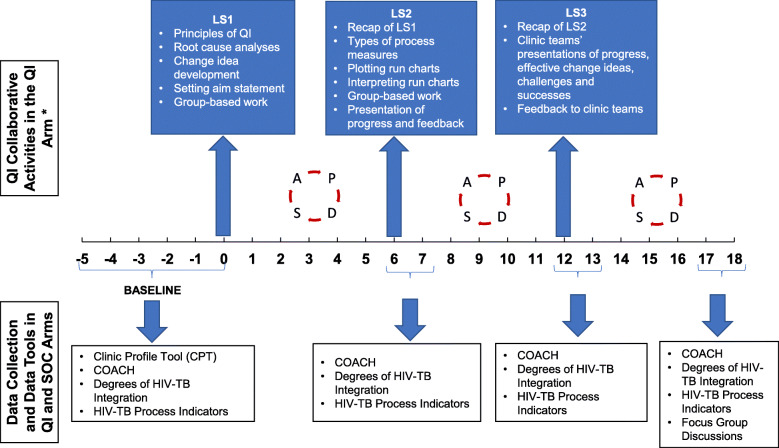
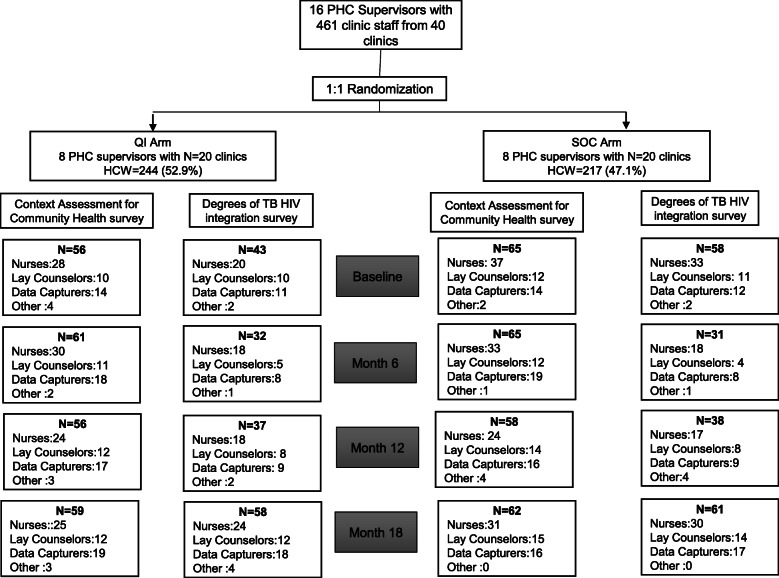
Methods: This is a nested sub-study embedded in a cluster-randomized controlled trial. Sixteen nurse supervisors (clusters) overseeing 40 clinics were randomized (1:1) to receive QI training and mentorship, or standard of care support (SOC). In the QI arm, eight nurse supervisors and 20 clinics formed a "collaborative" which aimed to improve HIV-TB process indicators, namely HIV testing, TB screening, isoniazid preventive therapy (IPT) initiations, viral load testing, and antiretroviral therapy for TB patients. OCFs measured at baseline were physical infrastructure, key staff, flexibility of clinic hours, monitoring data for improvement (MDI), and leadership support. Surveys were administered to clinic staff at baseline and month 12 to assess perceptions of supportiveness of contexts for change, and clinic organization for delivering integrated HIV-TB services. Linear mixed modelling was used to test for associations between OCFs and HIV-TB process indicators.
Results: A total of 209 clinic staff participated in the study; 97 (46.4%) and 112 (53.6%) from QI and SOC arms, respectively. There were no differences between the QI and SOC arms scores achieved for physical infrastructure (78.9% vs 64.7%; p = 0.058), key staff (95.8 vs 92; p = 0.270), clinic hours (66.9 vs 65.5; p = 0.900), MDI (63.3 vs 65; p = 0.875, leadership support (46.0 vs 57.4; p = 0.265), and perceptions of supportiveness of contexts for change (76.2 vs 79.7; p = 0.128 and clinic organization for delivering integrated HIV-TB services (74.1 vs 80.1; p = 0.916). IPT initiation was the only indicator that was significantly improved in the parent study. MDI was a significantly associated with increasing IPT initiation rates [beta coefficient (β) = 0.004; p = 0.004].
Discussion: MDI is a practice that should be fostered in public health facilities to increase the likelihood of success of future QI collaboratives to improve HIV-TB service delivery.
Trial registration: Clinicaltrials.gov , NCT02654613 . Registered 01 June 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


