Helen L Graham, Andrew Lac, Haeok Lee, Melissa J Benton
{"title":"预测心脏事件后的长期死亡率、发病率和生存结果:一项心脏康复研究。","authors":"Helen L Graham, Andrew Lac, Haeok Lee, Melissa J Benton","doi":"10.1177/1179572719827610","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac rehabilitation (CR) has been shown to decrease mortality and morbidity but estimations vary. While there is significant literature supporting short-term benefits, there is not a similarly body of research as to long-term (LT) benefits. Low participation rates in CR are due to several causes and evidence demonstrating positive LT outcomes could be a catalyst to increased participation rates.</p><p><strong>Objective: </strong>To predict LT mortality, readmission, and survival benefits associated with CR participation in a nationally certified program.</p><p><strong>Methods: </strong>Investigators collected mortality and hospital readmission data in a retrospective study to examine a cohort of cardiac patients following a myocardial infarction (MI), MI/percutaneous coronary intervention (PCI), and coronary artery bypass graft (CABG) up to 14 years ago. Hospital electronic medical record (EMR; n = 207) were used to measure hospital readmission outcome and State Health Department records (n = 361) for mortality and survival outcomes. Participation in CR, age, gender prior history of cardiac event, and diagnosis were used to predict readmission, mortality, and survival.</p><p><strong>Results: </strong>Approximately half (52.1%) the sample participated in CR. Participants included 72% males, average age 68 years (38-91 years), and were predominantly Non-Hispanic white. CR participants attended an average of 20 sessions. CR group differed in diagnoses MI (58.5%), CABG (57.4%) and in prior history of heart disease (25.4%) from the non-cardiac rehabilitation (NCR) group (83.2%, 25.4%, 42.2%, respectively) (<i>P</i> < .05). After controlling for the covariates in logistic regression analyses, the CR group independently predicted lower all-cause mortality (odds ratio, OR = 0.22, 95% CI 0.12 to 0.39) and decreased hospital readmissions (OR = 0.48, 95% CI 0.24 to 0.96). After controlling for the covariates in survival analysis, the CR group significantly contributed to decreased likelihood of death hazard (hazard ratio = 0.36, 95% CI 0.24 to 0.54). Median survivor time for the participants was 5.91 years, SD = 3.81 years.</p><p><strong>Conclusions: </strong>Participation in CR for middle age and elderly patients is associated with increased survival, a marked decrease in all-cause mortality, and a decrease in cardiovascular-related hospital readmission. A referral to a nationally certified outpatient CR program prior to hospital discharge and early enrollment may improve LT outcomes.</p>","PeriodicalId":41347,"journal":{"name":"Rehabilitation Process and Outcome","volume":"8 ","pages":"1179572719827610"},"PeriodicalIF":1.4000,"publicationDate":"2019-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179572719827610","citationCount":"10","resultStr":"{\"title\":\"Predicting Long-Term Mortality, Morbidity, and Survival Outcomes Following a Cardiac Event: A Cardiac Rehabilitation Study.\",\"authors\":\"Helen L Graham, Andrew Lac, Haeok Lee, Melissa J Benton\",\"doi\":\"10.1177/1179572719827610\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiac rehabilitation (CR) has been shown to decrease mortality and morbidity but estimations vary. While there is significant literature supporting short-term benefits, there is not a similarly body of research as to long-term (LT) benefits. Low participation rates in CR are due to several causes and evidence demonstrating positive LT outcomes could be a catalyst to increased participation rates.</p><p><strong>Objective: </strong>To predict LT mortality, readmission, and survival benefits associated with CR participation in a nationally certified program.</p><p><strong>Methods: </strong>Investigators collected mortality and hospital readmission data in a retrospective study to examine a cohort of cardiac patients following a myocardial infarction (MI), MI/percutaneous coronary intervention (PCI), and coronary artery bypass graft (CABG) up to 14 years ago. Hospital electronic medical record (EMR; n = 207) were used to measure hospital readmission outcome and State Health Department records (n = 361) for mortality and survival outcomes. Participation in CR, age, gender prior history of cardiac event, and diagnosis were used to predict readmission, mortality, and survival.</p><p><strong>Results: </strong>Approximately half (52.1%) the sample participated in CR. Participants included 72% males, average age 68 years (38-91 years), and were predominantly Non-Hispanic white. CR participants attended an average of 20 sessions. CR group differed in diagnoses MI (58.5%), CABG (57.4%) and in prior history of heart disease (25.4%) from the non-cardiac rehabilitation (NCR) group (83.2%, 25.4%, 42.2%, respectively) (<i>P</i> < .05). After controlling for the covariates in logistic regression analyses, the CR group independently predicted lower all-cause mortality (odds ratio, OR = 0.22, 95% CI 0.12 to 0.39) and decreased hospital readmissions (OR = 0.48, 95% CI 0.24 to 0.96). After controlling for the covariates in survival analysis, the CR group significantly contributed to decreased likelihood of death hazard (hazard ratio = 0.36, 95% CI 0.24 to 0.54). Median survivor time for the participants was 5.91 years, SD = 3.81 years.</p><p><strong>Conclusions: </strong>Participation in CR for middle age and elderly patients is associated with increased survival, a marked decrease in all-cause mortality, and a decrease in cardiovascular-related hospital readmission. A referral to a nationally certified outpatient CR program prior to hospital discharge and early enrollment may improve LT outcomes.</p>\",\"PeriodicalId\":41347,\"journal\":{\"name\":\"Rehabilitation Process and Outcome\",\"volume\":\"8 \",\"pages\":\"1179572719827610\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2019-02-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179572719827610\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rehabilitation Process and Outcome\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179572719827610\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"REHABILITATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rehabilitation Process and Outcome","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179572719827610","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
Predicting Long-Term Mortality, Morbidity, and Survival Outcomes Following a Cardiac Event: A Cardiac Rehabilitation Study.
Background: Cardiac rehabilitation (CR) has been shown to decrease mortality and morbidity but estimations vary. While there is significant literature supporting short-term benefits, there is not a similarly body of research as to long-term (LT) benefits. Low participation rates in CR are due to several causes and evidence demonstrating positive LT outcomes could be a catalyst to increased participation rates.
Objective: To predict LT mortality, readmission, and survival benefits associated with CR participation in a nationally certified program.
Methods: Investigators collected mortality and hospital readmission data in a retrospective study to examine a cohort of cardiac patients following a myocardial infarction (MI), MI/percutaneous coronary intervention (PCI), and coronary artery bypass graft (CABG) up to 14 years ago. Hospital electronic medical record (EMR; n = 207) were used to measure hospital readmission outcome and State Health Department records (n = 361) for mortality and survival outcomes. Participation in CR, age, gender prior history of cardiac event, and diagnosis were used to predict readmission, mortality, and survival.
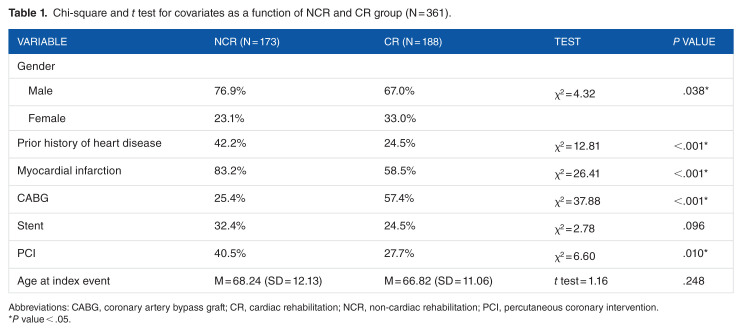
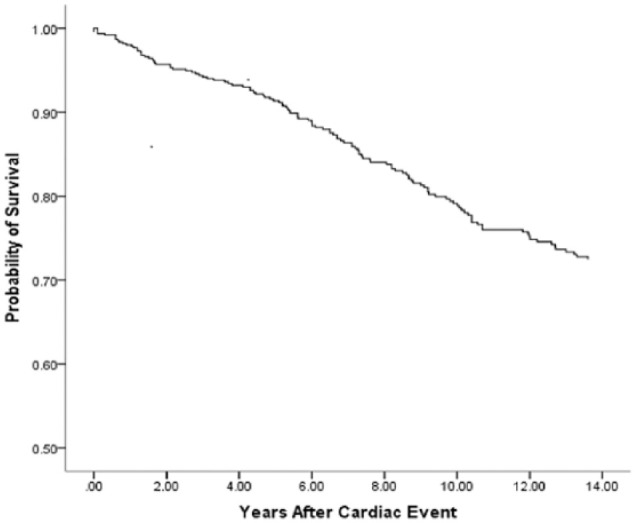
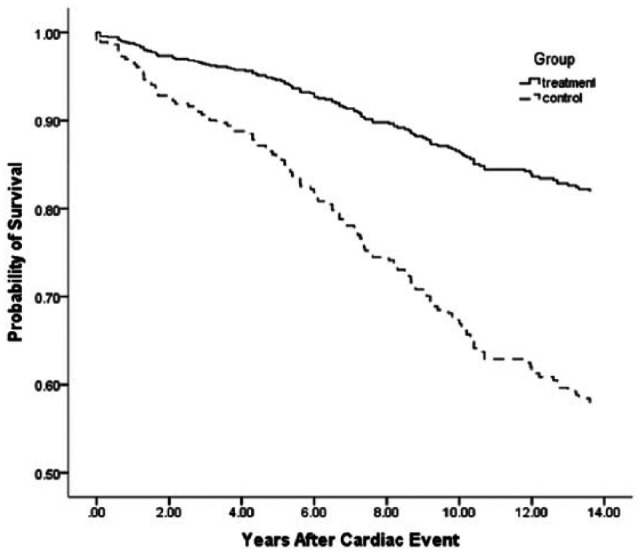
Results: Approximately half (52.1%) the sample participated in CR. Participants included 72% males, average age 68 years (38-91 years), and were predominantly Non-Hispanic white. CR participants attended an average of 20 sessions. CR group differed in diagnoses MI (58.5%), CABG (57.4%) and in prior history of heart disease (25.4%) from the non-cardiac rehabilitation (NCR) group (83.2%, 25.4%, 42.2%, respectively) (P < .05). After controlling for the covariates in logistic regression analyses, the CR group independently predicted lower all-cause mortality (odds ratio, OR = 0.22, 95% CI 0.12 to 0.39) and decreased hospital readmissions (OR = 0.48, 95% CI 0.24 to 0.96). After controlling for the covariates in survival analysis, the CR group significantly contributed to decreased likelihood of death hazard (hazard ratio = 0.36, 95% CI 0.24 to 0.54). Median survivor time for the participants was 5.91 years, SD = 3.81 years.
Conclusions: Participation in CR for middle age and elderly patients is associated with increased survival, a marked decrease in all-cause mortality, and a decrease in cardiovascular-related hospital readmission. A referral to a nationally certified outpatient CR program prior to hospital discharge and early enrollment may improve LT outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


