Boonphiphop Boonpheng, Panupong Hansrivijit, Charat Thongprayoon, Shennen A Mao, Pradeep K Vaitla, Tarun Bathini, Avishek Choudhury, Wisit Kaewput, Michael A Mao, Wisit Cheungpasitporn
{"title":"利妥昔单抗或血浆置换预防肾移植后局灶节段性肾小球硬化复发:一项系统回顾和荟萃分析。","authors":"Boonphiphop Boonpheng, Panupong Hansrivijit, Charat Thongprayoon, Shennen A Mao, Pradeep K Vaitla, Tarun Bathini, Avishek Choudhury, Wisit Kaewput, Michael A Mao, Wisit Cheungpasitporn","doi":"10.5500/wjt.v11.i7.303","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Focal segmental glomerulosclerosis (FSGS) is one of the most common glomerular diseases leading to renal failure. FSGS has a high risk of recurrence after kidney transplantation. Prevention of recurrent FSGS using rituximab and/or plasmapheresis has been evaluated in multiple small studies with conflicting results.</p><p><strong>Aim: </strong>To assess the risk of recurrence of FSGS after transplantation using prophylactic rituximab with or without plasmapheresis, and plasmapheresis alone compared to the standard treatment group without preventive therapy.</p><p><strong>Methods: </strong>This meta-analysis and systematic review were performed by first conducting a literature search of the MEDLINE, EMBASE, and Cochrane databases, from inception through March 2021; search terms included 'FSGS,' 'steroid-resistant nephrotic syndrome', 'rituximab,' and 'plasmapheresis,'. We identified studies that assessed the risk of post-transplant FSGS after use of rituximab with or without plasmapheresis, or plasmapheresis alone. Inclusion criteria were: Original, published, randomized controlled trials or cohort studies (either prospective or retrospective), case-control, or cross-sectional studies; inclusion of odds ratio, relative risk, and standardized incidence ratio with 95% confidence intervals (CI), or sufficient raw data to calculate these ratios; and subjects without interventions (controls) being used as comparators in cohort and cross-sectional studies. Effect estimates from individual studies were extracted and combined using a random effects model.</p><p><strong>Results: </strong>Eleven studies, with a total of 399 kidney transplant recipients with FSGS, evaluated the use of rituximab with or without plasmapheresis; thirteen studies, with a total of 571 kidney transplant recipients with FSGS, evaluated plasmapheresis alone. Post-transplant FSGS recurred relatively early. There was no significant difference in recurrence between the group that received rituximab (with or without plasmapheresis) and the standard treatment group, with a pooled risk ratio of 0.82 (95%CI: 0.47-1.45, <i>I</i> <sup>2</sup> = 65%). Similarly, plasmapheresis alone was not associated with any significant difference in FSGS recurrence when compared with no plasmapheresis; the pooled risk ratio was 0.85 (95%CI: 0.60-1.21, <i>I</i> <sup>2</sup> = 23%). Subgroup analyses in the pediatric and adult groups did not yield a significant difference in recurrence risk. We also reviewed and analyzed post-transplant outcomes including timing of recurrence and graft survival.</p><p><strong>Conclusion: </strong>Overall, the use of rituximab with or without plasmapheresis, or plasmapheresis alone, is not associated with a lower risk of FSGS recurrence after kidney transplantation. Future studies are required to assess the effectiveness of rituximab with or without plasmapheresis among specific patient subgroups with high-risk for FSGS recurrence.</p>","PeriodicalId":68893,"journal":{"name":"世界移植杂志(英文版)","volume":"11 7","pages":"303-319"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7b/43/WJT-11-303.PMC8291000.pdf","citationCount":"8","resultStr":"{\"title\":\"Rituximab or plasmapheresis for prevention of recurrent focal segmental glomerulosclerosis after kidney transplantation: A systematic review and meta-analysis.\",\"authors\":\"Boonphiphop Boonpheng, Panupong Hansrivijit, Charat Thongprayoon, Shennen A Mao, Pradeep K Vaitla, Tarun Bathini, Avishek Choudhury, Wisit Kaewput, Michael A Mao, Wisit Cheungpasitporn\",\"doi\":\"10.5500/wjt.v11.i7.303\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Focal segmental glomerulosclerosis (FSGS) is one of the most common glomerular diseases leading to renal failure. FSGS has a high risk of recurrence after kidney transplantation. Prevention of recurrent FSGS using rituximab and/or plasmapheresis has been evaluated in multiple small studies with conflicting results.</p><p><strong>Aim: </strong>To assess the risk of recurrence of FSGS after transplantation using prophylactic rituximab with or without plasmapheresis, and plasmapheresis alone compared to the standard treatment group without preventive therapy.</p><p><strong>Methods: </strong>This meta-analysis and systematic review were performed by first conducting a literature search of the MEDLINE, EMBASE, and Cochrane databases, from inception through March 2021; search terms included 'FSGS,' 'steroid-resistant nephrotic syndrome', 'rituximab,' and 'plasmapheresis,'. We identified studies that assessed the risk of post-transplant FSGS after use of rituximab with or without plasmapheresis, or plasmapheresis alone. Inclusion criteria were: Original, published, randomized controlled trials or cohort studies (either prospective or retrospective), case-control, or cross-sectional studies; inclusion of odds ratio, relative risk, and standardized incidence ratio with 95% confidence intervals (CI), or sufficient raw data to calculate these ratios; and subjects without interventions (controls) being used as comparators in cohort and cross-sectional studies. Effect estimates from individual studies were extracted and combined using a random effects model.</p><p><strong>Results: </strong>Eleven studies, with a total of 399 kidney transplant recipients with FSGS, evaluated the use of rituximab with or without plasmapheresis; thirteen studies, with a total of 571 kidney transplant recipients with FSGS, evaluated plasmapheresis alone. Post-transplant FSGS recurred relatively early. There was no significant difference in recurrence between the group that received rituximab (with or without plasmapheresis) and the standard treatment group, with a pooled risk ratio of 0.82 (95%CI: 0.47-1.45, <i>I</i> <sup>2</sup> = 65%). Similarly, plasmapheresis alone was not associated with any significant difference in FSGS recurrence when compared with no plasmapheresis; the pooled risk ratio was 0.85 (95%CI: 0.60-1.21, <i>I</i> <sup>2</sup> = 23%). Subgroup analyses in the pediatric and adult groups did not yield a significant difference in recurrence risk. We also reviewed and analyzed post-transplant outcomes including timing of recurrence and graft survival.</p><p><strong>Conclusion: </strong>Overall, the use of rituximab with or without plasmapheresis, or plasmapheresis alone, is not associated with a lower risk of FSGS recurrence after kidney transplantation. Future studies are required to assess the effectiveness of rituximab with or without plasmapheresis among specific patient subgroups with high-risk for FSGS recurrence.</p>\",\"PeriodicalId\":68893,\"journal\":{\"name\":\"世界移植杂志(英文版)\",\"volume\":\"11 7\",\"pages\":\"303-319\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7b/43/WJT-11-303.PMC8291000.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界移植杂志(英文版)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5500/wjt.v11.i7.303\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5500/wjt.v11.i7.303","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Rituximab or plasmapheresis for prevention of recurrent focal segmental glomerulosclerosis after kidney transplantation: A systematic review and meta-analysis.
Background: Focal segmental glomerulosclerosis (FSGS) is one of the most common glomerular diseases leading to renal failure. FSGS has a high risk of recurrence after kidney transplantation. Prevention of recurrent FSGS using rituximab and/or plasmapheresis has been evaluated in multiple small studies with conflicting results.
Aim: To assess the risk of recurrence of FSGS after transplantation using prophylactic rituximab with or without plasmapheresis, and plasmapheresis alone compared to the standard treatment group without preventive therapy.
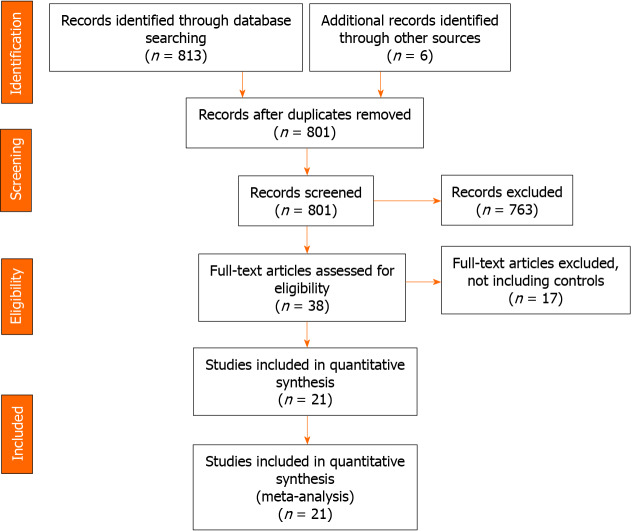
Methods: This meta-analysis and systematic review were performed by first conducting a literature search of the MEDLINE, EMBASE, and Cochrane databases, from inception through March 2021; search terms included 'FSGS,' 'steroid-resistant nephrotic syndrome', 'rituximab,' and 'plasmapheresis,'. We identified studies that assessed the risk of post-transplant FSGS after use of rituximab with or without plasmapheresis, or plasmapheresis alone. Inclusion criteria were: Original, published, randomized controlled trials or cohort studies (either prospective or retrospective), case-control, or cross-sectional studies; inclusion of odds ratio, relative risk, and standardized incidence ratio with 95% confidence intervals (CI), or sufficient raw data to calculate these ratios; and subjects without interventions (controls) being used as comparators in cohort and cross-sectional studies. Effect estimates from individual studies were extracted and combined using a random effects model.
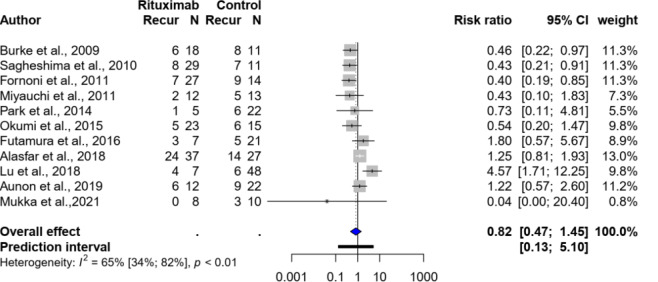
Results: Eleven studies, with a total of 399 kidney transplant recipients with FSGS, evaluated the use of rituximab with or without plasmapheresis; thirteen studies, with a total of 571 kidney transplant recipients with FSGS, evaluated plasmapheresis alone. Post-transplant FSGS recurred relatively early. There was no significant difference in recurrence between the group that received rituximab (with or without plasmapheresis) and the standard treatment group, with a pooled risk ratio of 0.82 (95%CI: 0.47-1.45, I2 = 65%). Similarly, plasmapheresis alone was not associated with any significant difference in FSGS recurrence when compared with no plasmapheresis; the pooled risk ratio was 0.85 (95%CI: 0.60-1.21, I2 = 23%). Subgroup analyses in the pediatric and adult groups did not yield a significant difference in recurrence risk. We also reviewed and analyzed post-transplant outcomes including timing of recurrence and graft survival.
Conclusion: Overall, the use of rituximab with or without plasmapheresis, or plasmapheresis alone, is not associated with a lower risk of FSGS recurrence after kidney transplantation. Future studies are required to assess the effectiveness of rituximab with or without plasmapheresis among specific patient subgroups with high-risk for FSGS recurrence.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


