Rui Caetano Oliveira, Maria João Martins, Carolina Moreno, Rui Almeida, João Carvalho, Paulo Teixeira, Miguel Teixeira, Edgar Tavares Silva, Isabel Paiva, Arnaldo Figueiredo, Maria Augusta Cipriano
{"title":"肾上腺皮质癌II期的组织学评分和肿瘤大小。","authors":"Rui Caetano Oliveira, Maria João Martins, Carolina Moreno, Rui Almeida, João Carvalho, Paulo Teixeira, Miguel Teixeira, Edgar Tavares Silva, Isabel Paiva, Arnaldo Figueiredo, Maria Augusta Cipriano","doi":"10.1177/20363613211026494","DOIUrl":null,"url":null,"abstract":"<p><p>Adrenocortical carcinomas (ACC) are aggressive tumors with a poor prognosis. Histological scores are advised for the diagnosis, however, there are borderline cases that may be misjudged as adrenocortical adenomas (ACA). The three main scores used are: Weiss Modified System (WMS), Reticulin Algorithm (RA), and Helsinki Score (HS). We intend to compare the accuracy of the three scores in ACC diagnosis and to identify predictive factors of overall survival (OS). Retrospective study (2004-2016) at Centro Hospitalar e Universitário de Coimbra of the adrenal tumors, classified as ACC or ACA, with a history of posterior tumor relapse/metastases, without lesions in the contralateral adrenal gland: 13F and 6M, with a median age of 51 ± 12.41 years. Nodules' median size was 9.20 ± 6.2 cm. Patients had a median OS of 52 ± 18.6 months, with 57.9% and 46.3%, at 3 and 5 years. Seven patients had local recurrence and nine had metastases. Thirteen cases were in stage II. The WMS and the HS allowed a diagnosis of ACC in 15 cases and the RA defined ACC in 17 cases. All cases had, at least, focal disruption of the reticulin framework. More than 5 mitosis/50 HPF was associated with worse OS: 49.67 ± 21.43 versus 108.86 ± 14.02 months (<i>p</i> = 0.026). In patients with stage II, tumor size ⩾10 cm was associated with worse OS: 19.25 ± 7.15 versus 96.11 ± 16.7 months (<i>p</i> = 0.007), confirmed by multivariate analysis (<i>p</i> = 0.031). The correct diagnosis of ACC is a pathologist responsibility. The RA seems the most accurate. Any loss of the reticulin framework should raise awareness for malignancy. In patients on stage II, a size ⩾10 cm is a predictor of worse prognosis.</p>","PeriodicalId":46078,"journal":{"name":"Rare Tumors","volume":" ","pages":"20363613211026494"},"PeriodicalIF":0.9000,"publicationDate":"2021-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/20363613211026494","citationCount":"1","resultStr":"{\"title\":\"Histological scores and tumor size on stage II in adrenocortical carcinomas.\",\"authors\":\"Rui Caetano Oliveira, Maria João Martins, Carolina Moreno, Rui Almeida, João Carvalho, Paulo Teixeira, Miguel Teixeira, Edgar Tavares Silva, Isabel Paiva, Arnaldo Figueiredo, Maria Augusta Cipriano\",\"doi\":\"10.1177/20363613211026494\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Adrenocortical carcinomas (ACC) are aggressive tumors with a poor prognosis. Histological scores are advised for the diagnosis, however, there are borderline cases that may be misjudged as adrenocortical adenomas (ACA). The three main scores used are: Weiss Modified System (WMS), Reticulin Algorithm (RA), and Helsinki Score (HS). We intend to compare the accuracy of the three scores in ACC diagnosis and to identify predictive factors of overall survival (OS). Retrospective study (2004-2016) at Centro Hospitalar e Universitário de Coimbra of the adrenal tumors, classified as ACC or ACA, with a history of posterior tumor relapse/metastases, without lesions in the contralateral adrenal gland: 13F and 6M, with a median age of 51 ± 12.41 years. Nodules' median size was 9.20 ± 6.2 cm. Patients had a median OS of 52 ± 18.6 months, with 57.9% and 46.3%, at 3 and 5 years. Seven patients had local recurrence and nine had metastases. Thirteen cases were in stage II. The WMS and the HS allowed a diagnosis of ACC in 15 cases and the RA defined ACC in 17 cases. All cases had, at least, focal disruption of the reticulin framework. More than 5 mitosis/50 HPF was associated with worse OS: 49.67 ± 21.43 versus 108.86 ± 14.02 months (<i>p</i> = 0.026). In patients with stage II, tumor size ⩾10 cm was associated with worse OS: 19.25 ± 7.15 versus 96.11 ± 16.7 months (<i>p</i> = 0.007), confirmed by multivariate analysis (<i>p</i> = 0.031). The correct diagnosis of ACC is a pathologist responsibility. The RA seems the most accurate. Any loss of the reticulin framework should raise awareness for malignancy. In patients on stage II, a size ⩾10 cm is a predictor of worse prognosis.</p>\",\"PeriodicalId\":46078,\"journal\":{\"name\":\"Rare Tumors\",\"volume\":\" \",\"pages\":\"20363613211026494\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2021-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/20363613211026494\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rare Tumors\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20363613211026494\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rare Tumors","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20363613211026494","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
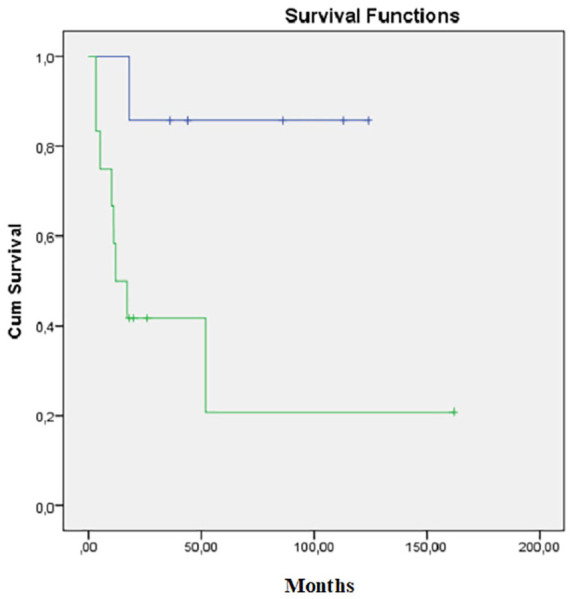
肾上腺皮质癌(ACC)是侵袭性肿瘤,预后差。组织学评分是诊断的建议,然而,也有可能被误诊为肾上腺皮质腺瘤(ACA)的边缘性病例。使用的三种主要评分是:Weiss Modified System (WMS)、Reticulin Algorithm (RA)和Helsinki Score (HS)。我们打算比较三种评分在ACC诊断中的准确性,并确定总生存期(OS)的预测因素。回顾性研究(2004-2016年)在Universitário de Coimbra中心医院进行的,分类为ACC或ACA,有肿瘤后侧复发/转移史,对侧肾上腺无病变的肾上腺肿瘤:13F和6M,中位年龄51±12.41岁。结节的中位大小为9.20±6.2 cm。患者在3年和5年的中位OS为52±18.6个月,分别为57.9%和46.3%。7例局部复发,9例转移。13例为II期。WMS和HS诊断ACC 15例,RA诊断ACC 17例。所有病例至少有局灶性网状结构破坏。超过5次有丝分裂/50 HPF与较差的OS相关:49.67±21.43 vs 108.86±14.02月(p = 0.026)。在II期患者中,肿瘤大小小于10 cm与更差的OS相关:19.25±7.15与96.11±16.7个月(p = 0.007),经多变量分析证实(p = 0.031)。正确诊断ACC是病理学家的责任。RA似乎是最准确的。网状蛋白框架的任何缺失都应提高对恶性肿瘤的认识。在II期患者中,小于10厘米是预后较差的预测因子。
Histological scores and tumor size on stage II in adrenocortical carcinomas.
Adrenocortical carcinomas (ACC) are aggressive tumors with a poor prognosis. Histological scores are advised for the diagnosis, however, there are borderline cases that may be misjudged as adrenocortical adenomas (ACA). The three main scores used are: Weiss Modified System (WMS), Reticulin Algorithm (RA), and Helsinki Score (HS). We intend to compare the accuracy of the three scores in ACC diagnosis and to identify predictive factors of overall survival (OS). Retrospective study (2004-2016) at Centro Hospitalar e Universitário de Coimbra of the adrenal tumors, classified as ACC or ACA, with a history of posterior tumor relapse/metastases, without lesions in the contralateral adrenal gland: 13F and 6M, with a median age of 51 ± 12.41 years. Nodules' median size was 9.20 ± 6.2 cm. Patients had a median OS of 52 ± 18.6 months, with 57.9% and 46.3%, at 3 and 5 years. Seven patients had local recurrence and nine had metastases. Thirteen cases were in stage II. The WMS and the HS allowed a diagnosis of ACC in 15 cases and the RA defined ACC in 17 cases. All cases had, at least, focal disruption of the reticulin framework. More than 5 mitosis/50 HPF was associated with worse OS: 49.67 ± 21.43 versus 108.86 ± 14.02 months (p = 0.026). In patients with stage II, tumor size ⩾10 cm was associated with worse OS: 19.25 ± 7.15 versus 96.11 ± 16.7 months (p = 0.007), confirmed by multivariate analysis (p = 0.031). The correct diagnosis of ACC is a pathologist responsibility. The RA seems the most accurate. Any loss of the reticulin framework should raise awareness for malignancy. In patients on stage II, a size ⩾10 cm is a predictor of worse prognosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


