Susan J Astley, Julia M Bledsoe, Julian K Davies, John C Thorne
{"title":"FASD 4位代码与homme等人2016年FASD诊断指南的比较。","authors":"Susan J Astley, Julia M Bledsoe, Julian K Davies, John C Thorne","doi":"10.12715/apr.2017.4.13","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>As clinicians strive to achieve consensus worldwide on how best to diagnose fetal alcohol spectrum disorders (FASD), the most recent FASD diagnosstic systems exhibit convergence and divergence. Applying these systems to a single clinical population illustrates contrasts between them, but validation studies are ultimately required to identify the best system. Currently, only the 4-Digit Code has published comprehensive validation studies.</p><p><strong>Methods: </strong>The 4-Digit Code and Hoyme 2016 FASD systems were applied to the records of 1,392 patients evaluated for FASD at the University of Washington to: 1) Compare the diagnostic criteria and tools used by each system, 2) Compare the prevalence and concordance of diagnostic outcomes and assess measures of validity.</p><p><strong>Results: </strong>Only 38% of patients received concordant diagnoses. The Hoyme criteria rendered half as many diagnoses under the umbrella of FASD (n=558) as the 4-Digit Code (n=1,092) and diagnosed a much higher proportion (53%) as fetal alcohol syndrome/partial fetal alcohol syndrome (FAS/PFAS) than the 4-Digit Code (7%). Key Hoyme factors contributing to discordance included relaxation of facial criteria (40% had the Hoyme FAS face, including patients with confirmed absence of alcohol exposure); setting alcohol exposure thresholds prevented 1/3 with confirmed exposure from receiving FAS/FASD diagnoses; and setting minimum age limits for Alcohol-Related Neurodevelopmental Disorder prevented 79% of alcohol-exposed infants with neurodevelopmental impairment a FASD diagnosis. The Hoyme Lip/Philtrum Guides differ substantively from the 4-Digit Lip-Philtrum Guides and thus are not valid for use with the 4-Digit Code.</p><p><strong>Conclusions: </strong>All FASD diagnostic systems need to publish comprehensive validation studies to identify which is the most accurate, reproducible, and medically valid.</p>","PeriodicalId":72104,"journal":{"name":"Advances in pediatric research","volume":"4 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7785113/pdf/","citationCount":"12","resultStr":"{\"title\":\"Comparison of the FASD 4-Digit Code and Hoyme et al. 2016 FASD diagnostic guidelines.\",\"authors\":\"Susan J Astley, Julia M Bledsoe, Julian K Davies, John C Thorne\",\"doi\":\"10.12715/apr.2017.4.13\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>As clinicians strive to achieve consensus worldwide on how best to diagnose fetal alcohol spectrum disorders (FASD), the most recent FASD diagnosstic systems exhibit convergence and divergence. Applying these systems to a single clinical population illustrates contrasts between them, but validation studies are ultimately required to identify the best system. Currently, only the 4-Digit Code has published comprehensive validation studies.</p><p><strong>Methods: </strong>The 4-Digit Code and Hoyme 2016 FASD systems were applied to the records of 1,392 patients evaluated for FASD at the University of Washington to: 1) Compare the diagnostic criteria and tools used by each system, 2) Compare the prevalence and concordance of diagnostic outcomes and assess measures of validity.</p><p><strong>Results: </strong>Only 38% of patients received concordant diagnoses. The Hoyme criteria rendered half as many diagnoses under the umbrella of FASD (n=558) as the 4-Digit Code (n=1,092) and diagnosed a much higher proportion (53%) as fetal alcohol syndrome/partial fetal alcohol syndrome (FAS/PFAS) than the 4-Digit Code (7%). Key Hoyme factors contributing to discordance included relaxation of facial criteria (40% had the Hoyme FAS face, including patients with confirmed absence of alcohol exposure); setting alcohol exposure thresholds prevented 1/3 with confirmed exposure from receiving FAS/FASD diagnoses; and setting minimum age limits for Alcohol-Related Neurodevelopmental Disorder prevented 79% of alcohol-exposed infants with neurodevelopmental impairment a FASD diagnosis. The Hoyme Lip/Philtrum Guides differ substantively from the 4-Digit Lip-Philtrum Guides and thus are not valid for use with the 4-Digit Code.</p><p><strong>Conclusions: </strong>All FASD diagnostic systems need to publish comprehensive validation studies to identify which is the most accurate, reproducible, and medically valid.</p>\",\"PeriodicalId\":72104,\"journal\":{\"name\":\"Advances in pediatric research\",\"volume\":\"4 3\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7785113/pdf/\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in pediatric research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12715/apr.2017.4.13\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/10/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in pediatric research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12715/apr.2017.4.13","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/10/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Comparison of the FASD 4-Digit Code and Hoyme et al. 2016 FASD diagnostic guidelines.
Background: As clinicians strive to achieve consensus worldwide on how best to diagnose fetal alcohol spectrum disorders (FASD), the most recent FASD diagnosstic systems exhibit convergence and divergence. Applying these systems to a single clinical population illustrates contrasts between them, but validation studies are ultimately required to identify the best system. Currently, only the 4-Digit Code has published comprehensive validation studies.
Methods: The 4-Digit Code and Hoyme 2016 FASD systems were applied to the records of 1,392 patients evaluated for FASD at the University of Washington to: 1) Compare the diagnostic criteria and tools used by each system, 2) Compare the prevalence and concordance of diagnostic outcomes and assess measures of validity.
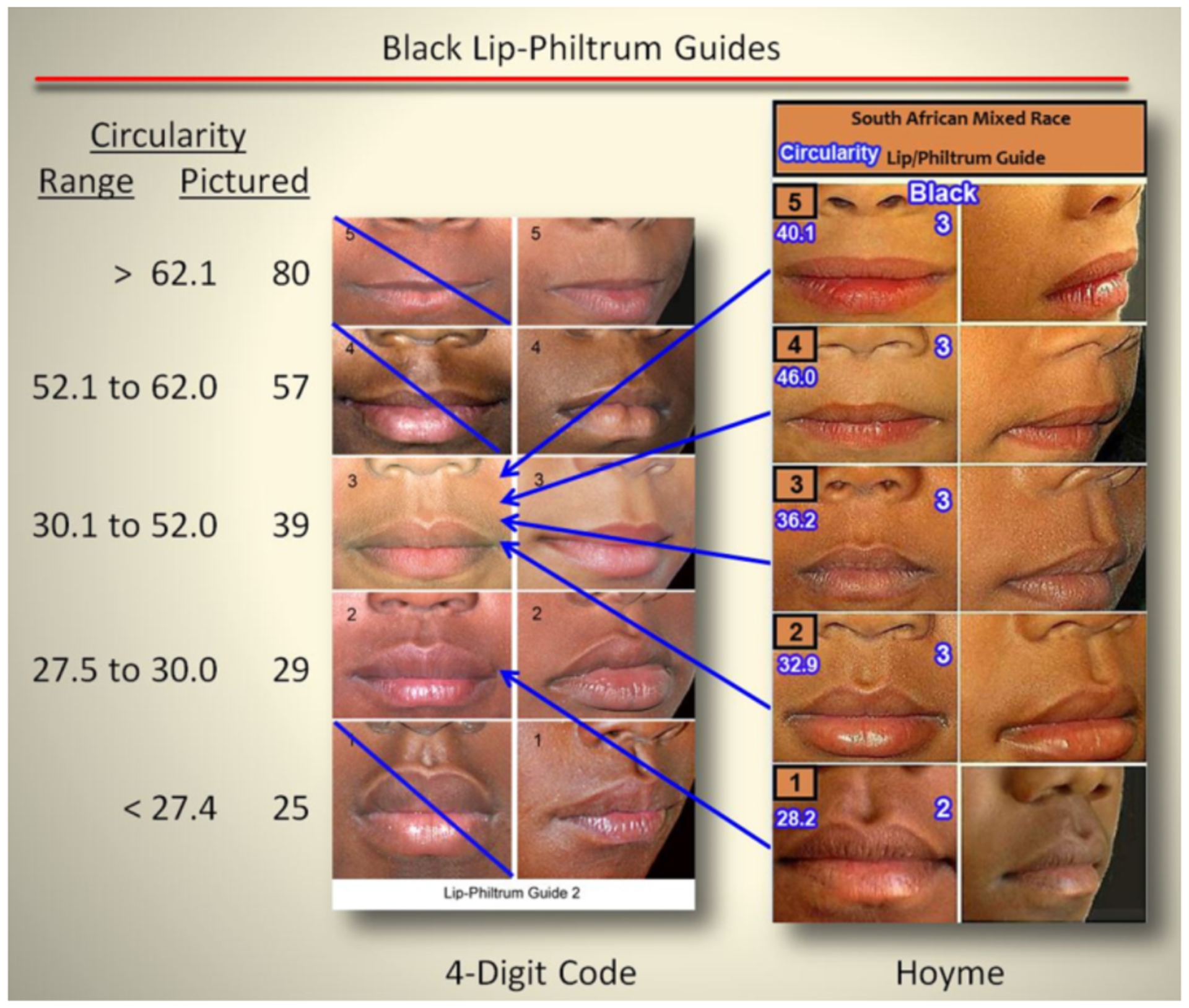
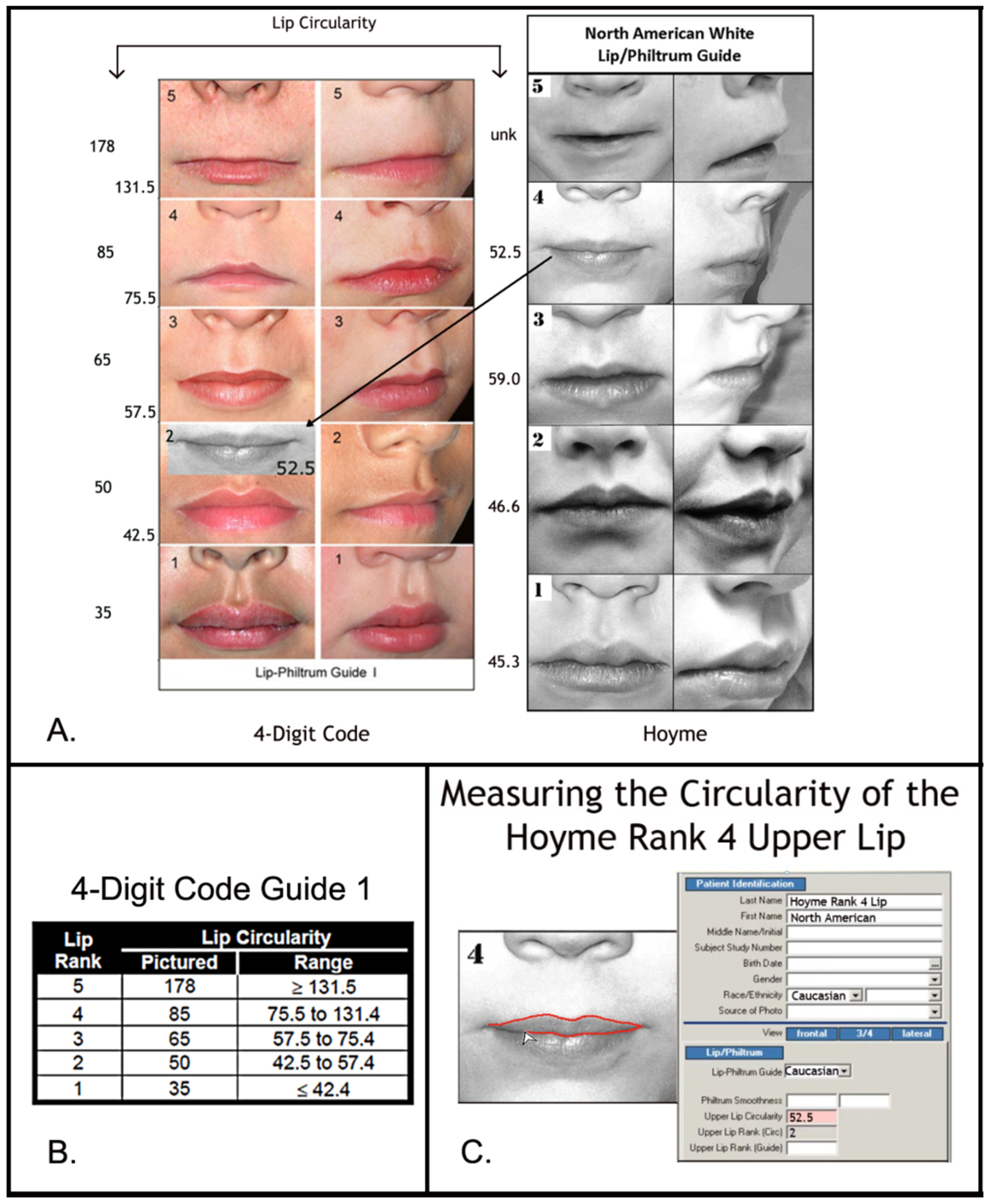
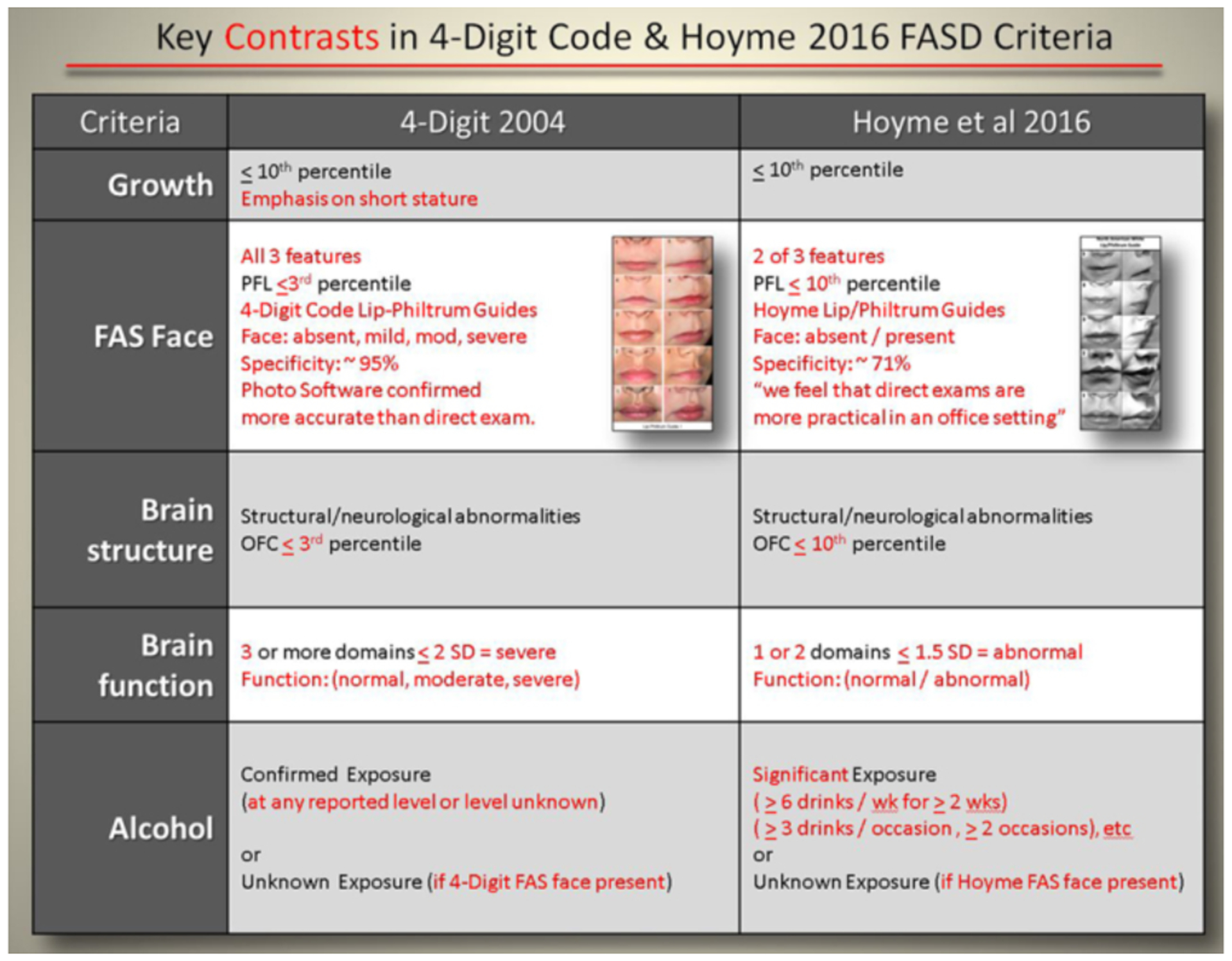
Results: Only 38% of patients received concordant diagnoses. The Hoyme criteria rendered half as many diagnoses under the umbrella of FASD (n=558) as the 4-Digit Code (n=1,092) and diagnosed a much higher proportion (53%) as fetal alcohol syndrome/partial fetal alcohol syndrome (FAS/PFAS) than the 4-Digit Code (7%). Key Hoyme factors contributing to discordance included relaxation of facial criteria (40% had the Hoyme FAS face, including patients with confirmed absence of alcohol exposure); setting alcohol exposure thresholds prevented 1/3 with confirmed exposure from receiving FAS/FASD diagnoses; and setting minimum age limits for Alcohol-Related Neurodevelopmental Disorder prevented 79% of alcohol-exposed infants with neurodevelopmental impairment a FASD diagnosis. The Hoyme Lip/Philtrum Guides differ substantively from the 4-Digit Lip-Philtrum Guides and thus are not valid for use with the 4-Digit Code.
Conclusions: All FASD diagnostic systems need to publish comprehensive validation studies to identify which is the most accurate, reproducible, and medically valid.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


