{"title":"鼻腔乙酰水杨酸挑战能否预测非甾体抗炎药(NSAIDs)加重呼吸系统疾病(N-ERD)的严重程度?","authors":"Ulrike Förster-Ruhrmann, Anne-Kristin Tietz, Jonghui Kim, Uta Liebers, Agnieszka J Szczepek, Heidi Olze","doi":"10.5414/ALX01996E","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-steroidal anti-inflammatory drugs (NSAIDs)-exacerbated respiratory disease (N-ERD) complicates the clinical course of chronic rhinosinusitis with nasal polyps (CRSwNP) and severe asthma. We aimed to determine the detection rate of NERD in patients with CRSwNP, asthma, and history of NSAID intolerance using nasal challenge with acetylsalicylic acid (ASA) and the relationship between the severities of response to ASA challenges and the grade of N-ERD.</p><p><strong>Materials and methods: </strong>Three groups of patients were included: CRSwNP with asthma and clinical history of analgesics intolerance (CRSwNP-AAI n = 18), CRSwNP with asthma but without a clinical history of analgesics intolerance (CRSwNP-A n = 20), and CRSwNP without asthma or analgesics intolerance (n = 18). All subjects were challenged nasally with 16 mg ASA and monitored with active anterior rhinomanometry. Rhinological (nasal polyp score), pulmonary (spirometry, Asthma Control Test (ACT), and asthma treatment), and psychometric questionnaire scores were recorded and correlated with rhinomanometric data following nasal challenges (flow depressions and symptom scores).</p><p><strong>Results: </strong>Nasal ASA challenge detected N-ERD in 96.7% of CRSwNP-AAI patients and 45% of CRSwNP-A patients. No N-ERD was seen in the CRSwNP group. The control grade of asthma measured with ACT scores was significantly lower in the groups CRSwNP-AAI (MV 18.22) and CRSwNP-A (MV 19.75) when compared to the CRSwNP group (MV 24.39) (p = 0.000). In the CRSwNP-AAI group, 11 patients had uncontrolled asthma (61%), and in the CRSwNP-A group, 9 patients had uncontrolled asthma (45%). No correlation was found between rhinology and pulmonary parameters, nasal symptoms, and the severity of nasal ASA challenges. Specific reactions were detectable under the therapy of prednisolone and omalizumab.</p><p><strong>Conclusion: </strong>N-ERD might not always be detected by screening a patient's medical history. Nasal ASA challenges are recommended in patients with CRSwNP and asthma. The nasal challenge with ASA positively confirms the N-ERD diagnosis. Moreover, N-ERD is a differential diagnosis in patients with severe asthma with the need for prednisolone or omalizumab therapy. The severity of the reaction to the ASA challenge in controlled and uncontrolled asthma patients is independent of the grade of N-ERD.\u2029.</p>","PeriodicalId":7485,"journal":{"name":"Allergologie Select","volume":"4 ","pages":"135-143"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7771579/pdf/","citationCount":"0","resultStr":"{\"title\":\"Can nasal acetylsalicylic acid challenge predict the severity of non-steroidal anti-inflammatory drugs (NSAIDs)-exacerbated respiratory disease (N-ERD)?\\u2029.\",\"authors\":\"Ulrike Förster-Ruhrmann, Anne-Kristin Tietz, Jonghui Kim, Uta Liebers, Agnieszka J Szczepek, Heidi Olze\",\"doi\":\"10.5414/ALX01996E\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Non-steroidal anti-inflammatory drugs (NSAIDs)-exacerbated respiratory disease (N-ERD) complicates the clinical course of chronic rhinosinusitis with nasal polyps (CRSwNP) and severe asthma. We aimed to determine the detection rate of NERD in patients with CRSwNP, asthma, and history of NSAID intolerance using nasal challenge with acetylsalicylic acid (ASA) and the relationship between the severities of response to ASA challenges and the grade of N-ERD.</p><p><strong>Materials and methods: </strong>Three groups of patients were included: CRSwNP with asthma and clinical history of analgesics intolerance (CRSwNP-AAI n = 18), CRSwNP with asthma but without a clinical history of analgesics intolerance (CRSwNP-A n = 20), and CRSwNP without asthma or analgesics intolerance (n = 18). All subjects were challenged nasally with 16 mg ASA and monitored with active anterior rhinomanometry. Rhinological (nasal polyp score), pulmonary (spirometry, Asthma Control Test (ACT), and asthma treatment), and psychometric questionnaire scores were recorded and correlated with rhinomanometric data following nasal challenges (flow depressions and symptom scores).</p><p><strong>Results: </strong>Nasal ASA challenge detected N-ERD in 96.7% of CRSwNP-AAI patients and 45% of CRSwNP-A patients. No N-ERD was seen in the CRSwNP group. The control grade of asthma measured with ACT scores was significantly lower in the groups CRSwNP-AAI (MV 18.22) and CRSwNP-A (MV 19.75) when compared to the CRSwNP group (MV 24.39) (p = 0.000). In the CRSwNP-AAI group, 11 patients had uncontrolled asthma (61%), and in the CRSwNP-A group, 9 patients had uncontrolled asthma (45%). No correlation was found between rhinology and pulmonary parameters, nasal symptoms, and the severity of nasal ASA challenges. Specific reactions were detectable under the therapy of prednisolone and omalizumab.</p><p><strong>Conclusion: </strong>N-ERD might not always be detected by screening a patient's medical history. Nasal ASA challenges are recommended in patients with CRSwNP and asthma. The nasal challenge with ASA positively confirms the N-ERD diagnosis. Moreover, N-ERD is a differential diagnosis in patients with severe asthma with the need for prednisolone or omalizumab therapy. The severity of the reaction to the ASA challenge in controlled and uncontrolled asthma patients is independent of the grade of N-ERD.\\u2029.</p>\",\"PeriodicalId\":7485,\"journal\":{\"name\":\"Allergologie Select\",\"volume\":\"4 \",\"pages\":\"135-143\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-12-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7771579/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergologie Select\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/ALX01996E\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergologie Select","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/ALX01996E","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:非甾体抗炎药(NSAIDs)加重呼吸系统疾病(N-ERD)使慢性鼻窦炎伴鼻息肉(CRSwNP)和严重哮喘的临床病程复杂化。我们的目的是通过使用乙酰水杨酸(ASA)鼻腔刺激,确定CRSwNP、哮喘和NSAID不耐受史患者的NERD检出率,以及对ASA刺激的反应程度与N-ERD分级之间的关系。材料与方法:将有哮喘且有镇痛药不耐受临床史的CRSwNP患者(CRSwNP- aai n = 18)、有哮喘但无镇痛药不耐受临床史的CRSwNP患者(CRSwNP- aai n = 20)、无哮喘或镇痛药不耐受的CRSwNP患者(n = 18)分为三组。所有受试者用16毫克ASA进行鼻腔刺激,并采用主动前鼻测压法进行监测。记录鼻科(鼻息肉评分)、肺科(肺活量测定、哮喘控制测试(ACT)和哮喘治疗)和心理测量问卷得分,并将其与鼻腔挑战(血流抑制和症状评分)后的鼻测量数据相关联。结果:鼻腔ASA激发在96.7%的CRSwNP-AAI患者和45%的CRSwNP-A患者中检测到N-ERD。CRSwNP组未见N-ERD。与CRSwNP组(MV 24.39)相比,CRSwNP- aai组(MV 18.22)和CRSwNP- a组(MV 19.75)的ACT评分的哮喘控制等级显著降低(p = 0.000)。在CRSwNP-AAI组中,11例患者哮喘未控制(61%),在CRSwNP-A组中,9例患者哮喘未控制(45%)。鼻科和肺部参数、鼻症状和鼻ASA挑战的严重程度之间没有发现相关性。在强的松龙和奥玛单抗治疗下可检测到特异性反应。结论:N-ERD可能并不总是通过筛查患者的病史而被发现。建议对CRSwNP和哮喘患者进行鼻腔ASA挑战。ASA鼻穿刺阳性证实了N-ERD的诊断。此外,N-ERD是需要强的松龙或奥玛珠单抗治疗的严重哮喘患者的鉴别诊断。对照和非对照哮喘患者对ASA挑战的反应严重程度与N-ERD的分级无关。 。
Can nasal acetylsalicylic acid challenge predict the severity of non-steroidal anti-inflammatory drugs (NSAIDs)-exacerbated respiratory disease (N-ERD)? .
Background: Non-steroidal anti-inflammatory drugs (NSAIDs)-exacerbated respiratory disease (N-ERD) complicates the clinical course of chronic rhinosinusitis with nasal polyps (CRSwNP) and severe asthma. We aimed to determine the detection rate of NERD in patients with CRSwNP, asthma, and history of NSAID intolerance using nasal challenge with acetylsalicylic acid (ASA) and the relationship between the severities of response to ASA challenges and the grade of N-ERD.
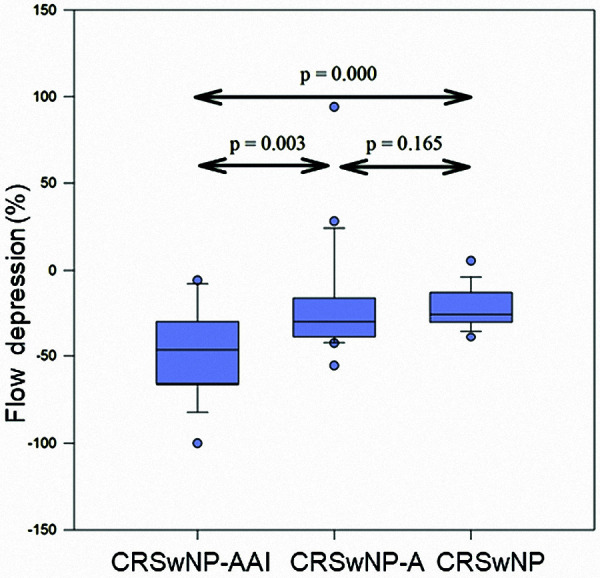
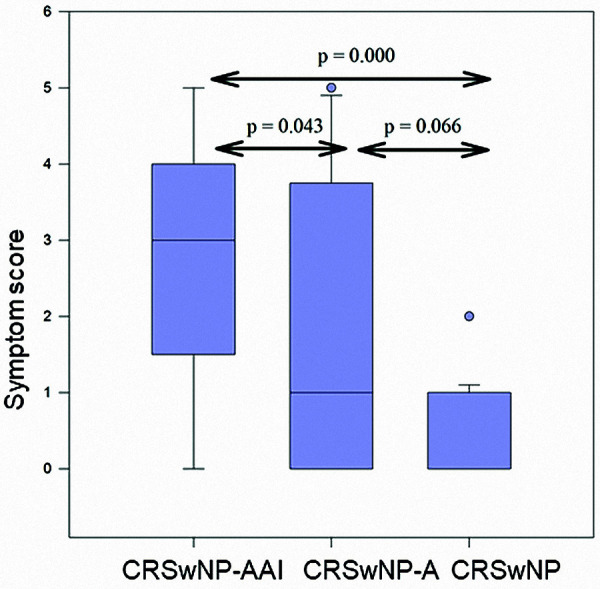
Materials and methods: Three groups of patients were included: CRSwNP with asthma and clinical history of analgesics intolerance (CRSwNP-AAI n = 18), CRSwNP with asthma but without a clinical history of analgesics intolerance (CRSwNP-A n = 20), and CRSwNP without asthma or analgesics intolerance (n = 18). All subjects were challenged nasally with 16 mg ASA and monitored with active anterior rhinomanometry. Rhinological (nasal polyp score), pulmonary (spirometry, Asthma Control Test (ACT), and asthma treatment), and psychometric questionnaire scores were recorded and correlated with rhinomanometric data following nasal challenges (flow depressions and symptom scores).
Results: Nasal ASA challenge detected N-ERD in 96.7% of CRSwNP-AAI patients and 45% of CRSwNP-A patients. No N-ERD was seen in the CRSwNP group. The control grade of asthma measured with ACT scores was significantly lower in the groups CRSwNP-AAI (MV 18.22) and CRSwNP-A (MV 19.75) when compared to the CRSwNP group (MV 24.39) (p = 0.000). In the CRSwNP-AAI group, 11 patients had uncontrolled asthma (61%), and in the CRSwNP-A group, 9 patients had uncontrolled asthma (45%). No correlation was found between rhinology and pulmonary parameters, nasal symptoms, and the severity of nasal ASA challenges. Specific reactions were detectable under the therapy of prednisolone and omalizumab.
Conclusion: N-ERD might not always be detected by screening a patient's medical history. Nasal ASA challenges are recommended in patients with CRSwNP and asthma. The nasal challenge with ASA positively confirms the N-ERD diagnosis. Moreover, N-ERD is a differential diagnosis in patients with severe asthma with the need for prednisolone or omalizumab therapy. The severity of the reaction to the ASA challenge in controlled and uncontrolled asthma patients is independent of the grade of N-ERD. .

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


