Carlos A Ordoñez, Michael W Parra, Mauricio Millán, Yaset Caicedo, Natalia Padilla, Alberto García, María Josefa Franco, Gonzalo Aristizábal, Luis Eduardo Toro, Luis Fernando Pino, Adolfo González-Hadad, Mario Alain Herrera, José Julián Serna, Fernando Rodríguez-Holguín, Alexander Salcedo, Claudia Orlas, Mónica Guzmán-Rodríguez, Fabian Hernández, Ricardo Ferrada, Rao Ivatury
{"title":"十二指肠穿透性创伤的损伤控制:越少越好--续集。","authors":"Carlos A Ordoñez, Michael W Parra, Mauricio Millán, Yaset Caicedo, Natalia Padilla, Alberto García, María Josefa Franco, Gonzalo Aristizábal, Luis Eduardo Toro, Luis Fernando Pino, Adolfo González-Hadad, Mario Alain Herrera, José Julián Serna, Fernando Rodríguez-Holguín, Alexander Salcedo, Claudia Orlas, Mónica Guzmán-Rodríguez, Fabian Hernández, Ricardo Ferrada, Rao Ivatury","doi":"10.25100/cm.v52i2.4509","DOIUrl":null,"url":null,"abstract":"<p><p>The overall incidence of duodenal injuries in severely injured trauma patients is between 0.2 to 0.6% and the overall prevalence in those suffering from abdominal trauma is 3 to 5%. Approximately 80% of these cases are secondary to penetrating trauma, commonly associated with vascular and adjacent organ injuries. Therefore, defining the best surgical treatment algorithm remains controversial. Mild to moderate duodenal trauma is currently managed via primary repair and simple surgical techniques. However, severe injuries have required complex surgical techniques without significant favorable outcomes and a consequential increase in mortality rates. This article aims to delineate the experience in the surgical management of penetrating duodenal injuries via the creation of a practical and effective algorithm that includes basic principles of damage control surgery that sticks to the philosophy of \"Less is Better\". Surgical management of all penetrating duodenal trauma should always default when possible to primary repair. When confronted with a complex duodenal injury, hemodynamic instability, and/or significant associated injuries, the default should be damage control surgery. Definitive reconstructive surgery should be postponed until the patient has been adequately resuscitated and the diamond of death has been corrected.</p>","PeriodicalId":50667,"journal":{"name":"Colombia Medica","volume":null,"pages":null},"PeriodicalIF":0.7000,"publicationDate":"2021-05-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/33/1657-9534-cm-52-02-e4104509.PMC8216054.pdf","citationCount":"0","resultStr":"{\"title\":\"Damage control in penetrating duodenal trauma: less is better - the sequel.\",\"authors\":\"Carlos A Ordoñez, Michael W Parra, Mauricio Millán, Yaset Caicedo, Natalia Padilla, Alberto García, María Josefa Franco, Gonzalo Aristizábal, Luis Eduardo Toro, Luis Fernando Pino, Adolfo González-Hadad, Mario Alain Herrera, José Julián Serna, Fernando Rodríguez-Holguín, Alexander Salcedo, Claudia Orlas, Mónica Guzmán-Rodríguez, Fabian Hernández, Ricardo Ferrada, Rao Ivatury\",\"doi\":\"10.25100/cm.v52i2.4509\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The overall incidence of duodenal injuries in severely injured trauma patients is between 0.2 to 0.6% and the overall prevalence in those suffering from abdominal trauma is 3 to 5%. Approximately 80% of these cases are secondary to penetrating trauma, commonly associated with vascular and adjacent organ injuries. Therefore, defining the best surgical treatment algorithm remains controversial. Mild to moderate duodenal trauma is currently managed via primary repair and simple surgical techniques. However, severe injuries have required complex surgical techniques without significant favorable outcomes and a consequential increase in mortality rates. This article aims to delineate the experience in the surgical management of penetrating duodenal injuries via the creation of a practical and effective algorithm that includes basic principles of damage control surgery that sticks to the philosophy of \\\"Less is Better\\\". Surgical management of all penetrating duodenal trauma should always default when possible to primary repair. When confronted with a complex duodenal injury, hemodynamic instability, and/or significant associated injuries, the default should be damage control surgery. Definitive reconstructive surgery should be postponed until the patient has been adequately resuscitated and the diamond of death has been corrected.</p>\",\"PeriodicalId\":50667,\"journal\":{\"name\":\"Colombia Medica\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2021-05-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/33/1657-9534-cm-52-02-e4104509.PMC8216054.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Colombia Medica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.25100/cm.v52i2.4509\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Colombia Medica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.25100/cm.v52i2.4509","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Damage control in penetrating duodenal trauma: less is better - the sequel.
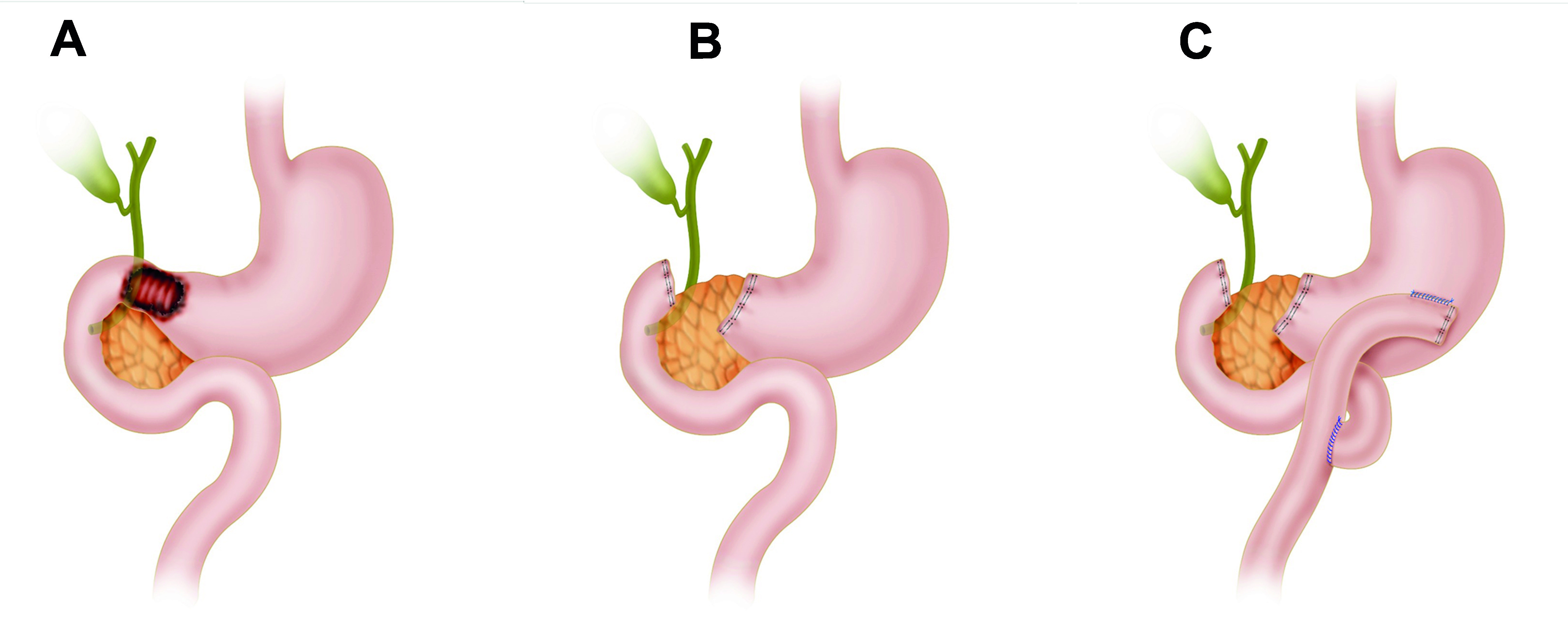
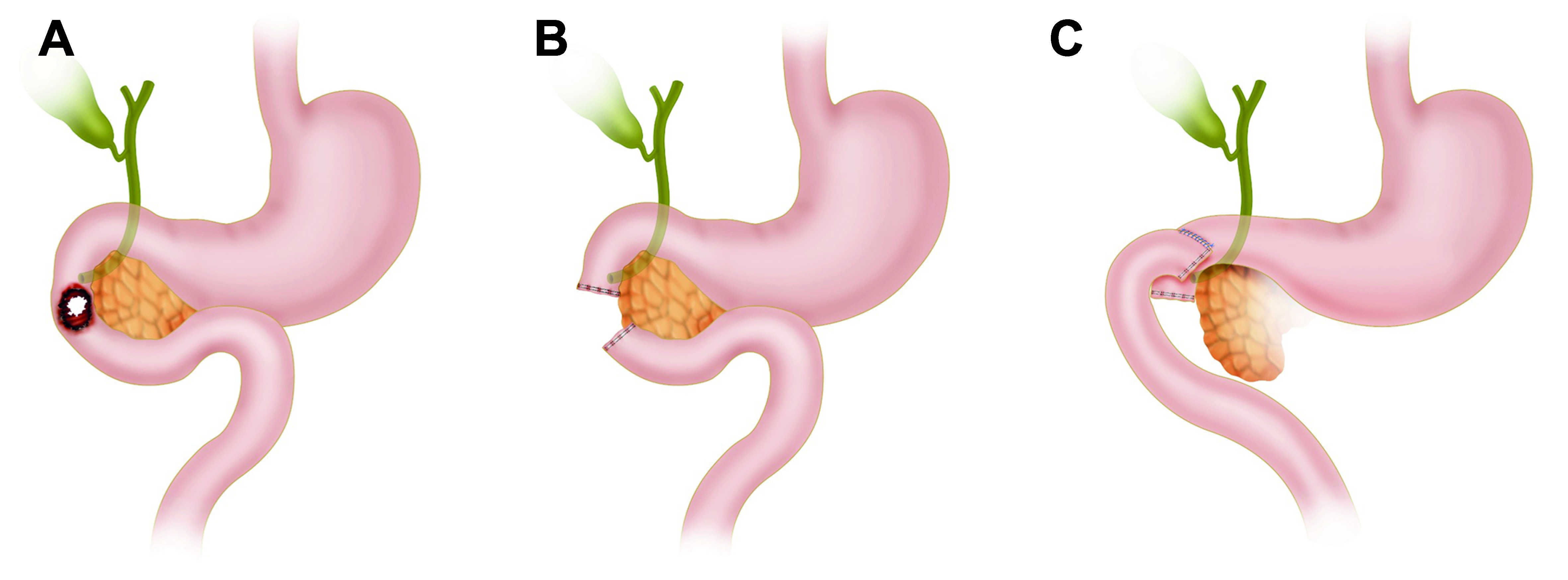
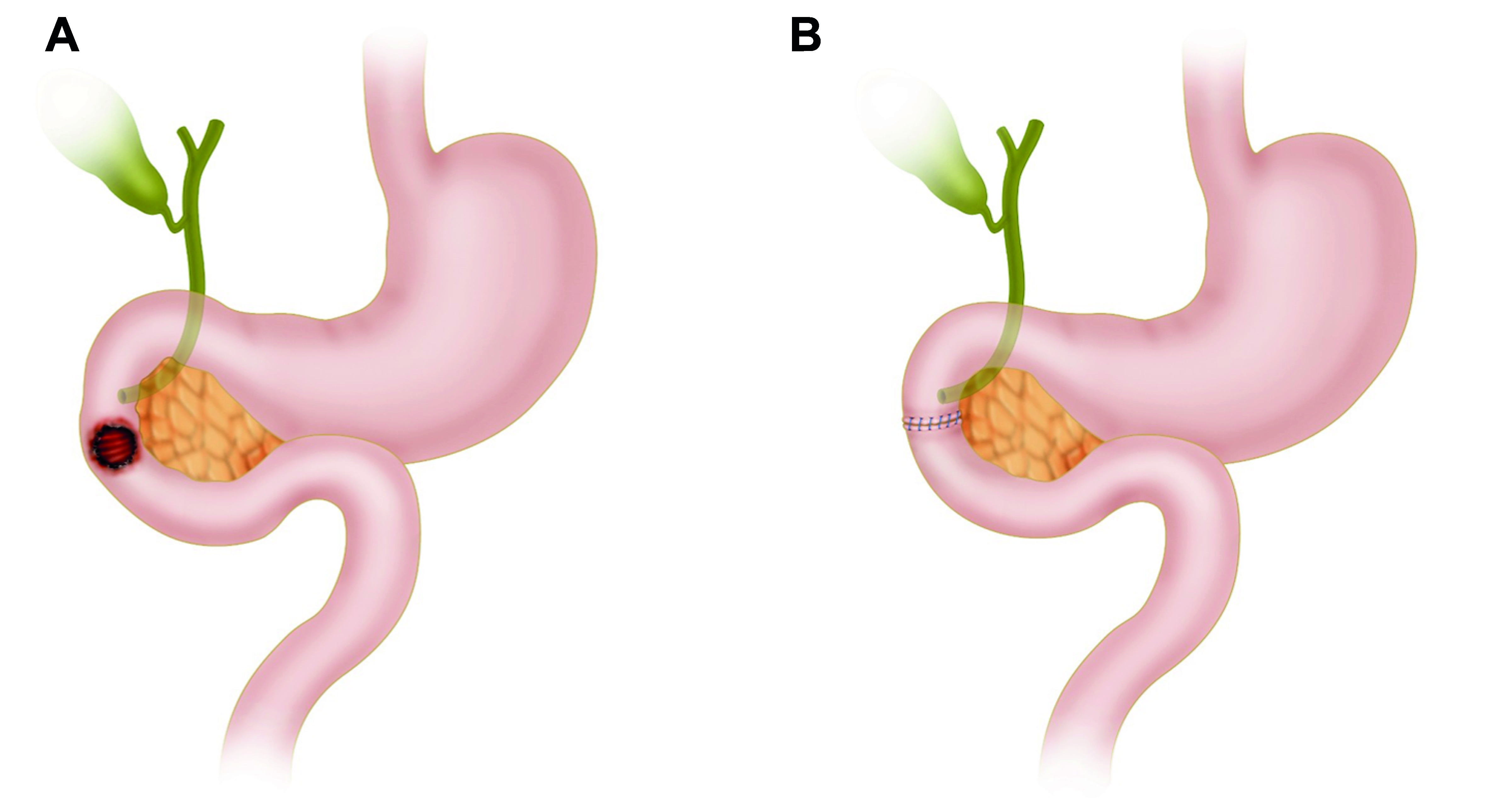
The overall incidence of duodenal injuries in severely injured trauma patients is between 0.2 to 0.6% and the overall prevalence in those suffering from abdominal trauma is 3 to 5%. Approximately 80% of these cases are secondary to penetrating trauma, commonly associated with vascular and adjacent organ injuries. Therefore, defining the best surgical treatment algorithm remains controversial. Mild to moderate duodenal trauma is currently managed via primary repair and simple surgical techniques. However, severe injuries have required complex surgical techniques without significant favorable outcomes and a consequential increase in mortality rates. This article aims to delineate the experience in the surgical management of penetrating duodenal injuries via the creation of a practical and effective algorithm that includes basic principles of damage control surgery that sticks to the philosophy of "Less is Better". Surgical management of all penetrating duodenal trauma should always default when possible to primary repair. When confronted with a complex duodenal injury, hemodynamic instability, and/or significant associated injuries, the default should be damage control surgery. Definitive reconstructive surgery should be postponed until the patient has been adequately resuscitated and the diamond of death has been corrected.
期刊介绍:
Colombia Médica is an international peer-reviewed medical journal that will consider any original contribution that advances or illuminates medical science or practice, or that educates to the journal''s’ readers.The journal is owned by a non-profit organization, Universidad del Valle, and serves the scientific community strictly following the International Committee of Medical Journal Editors (ICMJE) and the World Association of Medical Editors (WAME) recommendations of policies on publication ethics policies for medical journals.
Colombia Médica publishes original research articles, viewpoints and reviews in all areas of medical science and clinical practice. However, Colombia Médica gives the highest priority to papers on general and internal medicine, public health and primary health care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


