Job P van Kooten, Nadine L de Boer, Marjolein Diepeveen, Cornelis Verhoef, Jacobus W A Burger, Alexandra R M Brandt-Kerkhof, Eva V E Madsen
{"title":"经鼻胃造瘘管与经皮胃造瘘管在细胞减缩手术伴腹腔内高热化疗后预防性胃减压中的应用。","authors":"Job P van Kooten, Nadine L de Boer, Marjolein Diepeveen, Cornelis Verhoef, Jacobus W A Burger, Alexandra R M Brandt-Kerkhof, Eva V E Madsen","doi":"10.1515/pp-2021-0107","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is associated with postoperative gastroparesis and ileus. In 2015, our practice shifted from using percutaneous gastrostomy tubes (PGT), to nasogastric tubes (NGT) for prophylactic gastric decompression after CRS-HIPEC. This study aimed to compare these methods for length of stay (LOS) and associated complications.</p><p><strong>Methods: </strong>Patients that underwent CRS-HIPEC for peritoneal metastases from colorectal cancer between 2014 and 2019 were included. Cases were grouped based on receiving NGT or PGT postoperatively. Multivariable linear regression determined the independent effect of decompression method on LOS, thereby adjusting for confounders.</p><p><strong>Results: </strong>In total, 179 patients were included in the analyses. Median age was 64 years [IQR:54-71]. Altogether, 135 (75.4%) received a NGT and 44 (24.6%) received a PGT. Gastroparesis occurred significantly more often in the PGT group (18.2 vs. 7.4%, p=0.039). Median LOS was significantly shorter for patients with a NGT (15 [IQR:12-19] vs. 18.5 [IQR:17-25.5], p<0.001). PGT was independently associated with longer LOS in multivariable analysis (Beta=4.224 [95%CI 1.243-7.204]). There was no difference regarding aspiration, pneumonia and postoperative mortality between groups.</p><p><strong>Conclusions: </strong>NGT should be preferred over PGT for gastric decompression after CRS-HIPEC as it is associated with fewer gastroparesis and shorter LOS.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"6 2","pages":"57-65"},"PeriodicalIF":2.4000,"publicationDate":"2021-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1515/pp-2021-0107","citationCount":"0","resultStr":"{\"title\":\"Nasogastric- vs. percutaneous gastrostomy tube for prophylactic gastric decompression after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy.\",\"authors\":\"Job P van Kooten, Nadine L de Boer, Marjolein Diepeveen, Cornelis Verhoef, Jacobus W A Burger, Alexandra R M Brandt-Kerkhof, Eva V E Madsen\",\"doi\":\"10.1515/pp-2021-0107\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is associated with postoperative gastroparesis and ileus. In 2015, our practice shifted from using percutaneous gastrostomy tubes (PGT), to nasogastric tubes (NGT) for prophylactic gastric decompression after CRS-HIPEC. This study aimed to compare these methods for length of stay (LOS) and associated complications.</p><p><strong>Methods: </strong>Patients that underwent CRS-HIPEC for peritoneal metastases from colorectal cancer between 2014 and 2019 were included. Cases were grouped based on receiving NGT or PGT postoperatively. Multivariable linear regression determined the independent effect of decompression method on LOS, thereby adjusting for confounders.</p><p><strong>Results: </strong>In total, 179 patients were included in the analyses. Median age was 64 years [IQR:54-71]. Altogether, 135 (75.4%) received a NGT and 44 (24.6%) received a PGT. Gastroparesis occurred significantly more often in the PGT group (18.2 vs. 7.4%, p=0.039). Median LOS was significantly shorter for patients with a NGT (15 [IQR:12-19] vs. 18.5 [IQR:17-25.5], p<0.001). PGT was independently associated with longer LOS in multivariable analysis (Beta=4.224 [95%CI 1.243-7.204]). There was no difference regarding aspiration, pneumonia and postoperative mortality between groups.</p><p><strong>Conclusions: </strong>NGT should be preferred over PGT for gastric decompression after CRS-HIPEC as it is associated with fewer gastroparesis and shorter LOS.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"6 2\",\"pages\":\"57-65\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2021-03-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1515/pp-2021-0107\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2021-0107\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2021-0107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/6/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:细胞减少手术(CRS)联合腹腔热化疗(HIPEC)与术后胃轻瘫和肠梗阻有关。2015年,我们的做法从使用经皮胃造瘘管(PGT)转向鼻胃管(NGT)进行CRS-HIPEC术后预防性胃减压。本研究旨在比较这些方法的住院时间(LOS)和相关并发症。方法:纳入2014年至2019年期间接受CRS-HIPEC治疗的结直肠癌腹膜转移患者。根据术后接受NGT或PGT的情况进行分组。多变量线性回归确定了解压方法对LOS的独立影响,从而对混杂因素进行了调整。结果:共纳入179例患者。中位年龄64岁[IQR:54-71]。总共有135例(75.4%)接受了NGT, 44例(24.6%)接受了PGT。PGT组胃轻瘫的发生率明显高于对照组(18.2% vs. 7.4%, p=0.039)。NGT患者的中位LOS显著缩短(15 [IQR:12-19]对18.5 [IQR:17-25.5])。结论:在CRS-HIPEC术后,NGT应优先于PGT进行胃减压,因为它与胃轻瘫较少和LOS较短相关。
Nasogastric- vs. percutaneous gastrostomy tube for prophylactic gastric decompression after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy.
Objectives: Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is associated with postoperative gastroparesis and ileus. In 2015, our practice shifted from using percutaneous gastrostomy tubes (PGT), to nasogastric tubes (NGT) for prophylactic gastric decompression after CRS-HIPEC. This study aimed to compare these methods for length of stay (LOS) and associated complications.
Methods: Patients that underwent CRS-HIPEC for peritoneal metastases from colorectal cancer between 2014 and 2019 were included. Cases were grouped based on receiving NGT or PGT postoperatively. Multivariable linear regression determined the independent effect of decompression method on LOS, thereby adjusting for confounders.
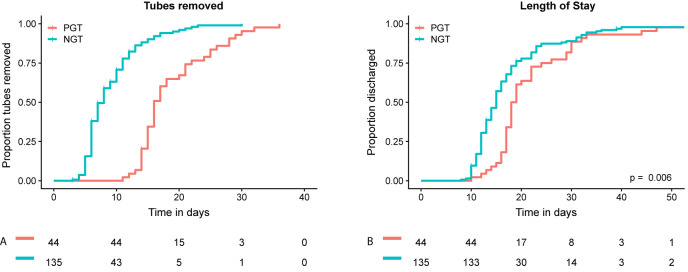
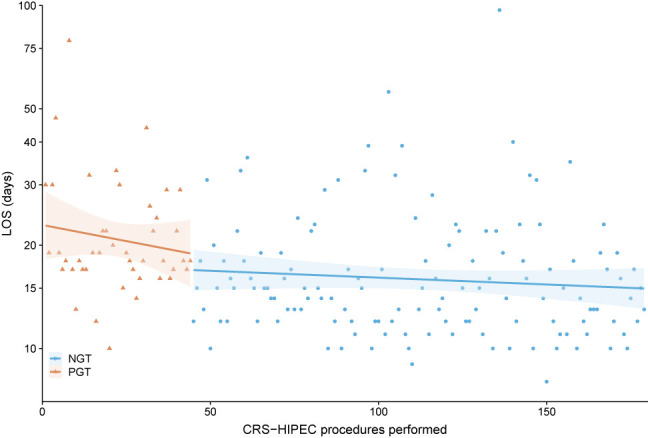
Results: In total, 179 patients were included in the analyses. Median age was 64 years [IQR:54-71]. Altogether, 135 (75.4%) received a NGT and 44 (24.6%) received a PGT. Gastroparesis occurred significantly more often in the PGT group (18.2 vs. 7.4%, p=0.039). Median LOS was significantly shorter for patients with a NGT (15 [IQR:12-19] vs. 18.5 [IQR:17-25.5], p<0.001). PGT was independently associated with longer LOS in multivariable analysis (Beta=4.224 [95%CI 1.243-7.204]). There was no difference regarding aspiration, pneumonia and postoperative mortality between groups.
Conclusions: NGT should be preferred over PGT for gastric decompression after CRS-HIPEC as it is associated with fewer gastroparesis and shorter LOS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


