Vanesa Anton-Vazquez, Paul Hine, Sanjeev Krishna, Marty Chaplin, Timothy Planche
{"title":"快速对照标准抗菌药物敏感性试验指导血流感染的治疗。","authors":"Vanesa Anton-Vazquez, Paul Hine, Sanjeev Krishna, Marty Chaplin, Timothy Planche","doi":"10.1002/14651858.CD013235.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rapid antimicrobial susceptibility tests are expected to reduce the time to clinically important results of a blood culture. This might enable clinicians to better target therapy to a person's needs, and thereby, improve health outcomes (mortality, length of hospital stay), and reduce unnecessary prescribing of broad-spectrum antibiotics; thereby reducing antimicrobial resistance rates.</p><p><strong>Objectives: </strong>To assess the effects of rapid susceptibility testing versus standard susceptibility testing for bloodstream infections (BSIs).</p><p><strong>Search methods: </strong>To identify studies with selected outcomes, we searched the Cochrane Infectious Diseases Group Specialised Register, CENTRAL, MEDLINE, LILACS, and two trials registries, between 1987 and October 2020. We used 'bloodstream infection' and 'antimicrobial susceptibility tests' as search terms. We had no language or publication status limitations.</p><p><strong>Selection criteria: </strong>Randomized controlled trials (RCTs) comparing rapid antimicrobial susceptibility testing (with a time-to-result of ≤ 8 hours) versus conventional antimicrobial susceptibility testing in people with a BSI caused by any bacteria, as identified by a positive blood culture.</p><p><strong>Data collection and analysis: </strong>Two review authors independently screened references, full-text reports of potentially relevant studies, extracted data from the studies, and assessed risk of bias. Any disagreement was discussed and resolved with a third review author. For mortality, a dichotomous outcome, we extracted the number of events in each arm, and presented a risk ratio (RR) with 95% confidence interval (CI) to compare rapid susceptibility testing to conventional methods. We used Review Manager 5.4 to meta-analyse the data. For other outcomes, which are time-to-event outcomes (time-to-discharge from hospital, time-to-first appropriate antibiotic change), we conducted qualitative narrative synthesis, due to heterogeneity of outcome measures. MAIN RESULTS: We included six trials, with 1638 participants. For rapid antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.10, 95% CI 0.82 to 1.46; 6 RCTs, 1638 participants; low-certainty evidence). In subgroup analysis, for rapid genotypic or molecular antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.02, 95% CI 0.69 to 1.49; 4 RCTs, 1074 participants; low-certainty evidence). For phenotypic rapid susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.37, 95% CI 0.80 to 2.35; 2 RCTs, 564 participants; low-certainty evidence). In qualitative analysis, rapid susceptibility testing may make little or no difference in time-to-discharge (4 RCTs, 1165 participants; low-certainty evidence). In qualitative analysis, rapid genotypic susceptibility testing compared to conventional testing may make little or no difference in time-to-appropriate antibiotic (3 RCTs, 929 participants; low-certainty evidence). In subgroup analysis, rapid phenotypic susceptibility testing compared to conventional testing may improve time-to-appropriate antibiotic (RR -17.29, CI -45.05 to 10.47; 2 RCTs, 564 participants; low-certainty evidence). AUTHORS' CONCLUSIONS: The theoretical benefits of rapid susceptibility testing have not been demonstrated to directly improve mortality, time-to-discharge, or time-to-appropriate antibiotic in these randomized studies. Future large prospective studies should be designed to focus on the most clinically meaningful outcomes, and aim to optimize blood culture pathways.</p>","PeriodicalId":515753,"journal":{"name":"The Cochrane database of systematic reviews","volume":" ","pages":"CD013235"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/14651858.CD013235.pub2","citationCount":"16","resultStr":"{\"title\":\"Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection.\",\"authors\":\"Vanesa Anton-Vazquez, Paul Hine, Sanjeev Krishna, Marty Chaplin, Timothy Planche\",\"doi\":\"10.1002/14651858.CD013235.pub2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Rapid antimicrobial susceptibility tests are expected to reduce the time to clinically important results of a blood culture. This might enable clinicians to better target therapy to a person's needs, and thereby, improve health outcomes (mortality, length of hospital stay), and reduce unnecessary prescribing of broad-spectrum antibiotics; thereby reducing antimicrobial resistance rates.</p><p><strong>Objectives: </strong>To assess the effects of rapid susceptibility testing versus standard susceptibility testing for bloodstream infections (BSIs).</p><p><strong>Search methods: </strong>To identify studies with selected outcomes, we searched the Cochrane Infectious Diseases Group Specialised Register, CENTRAL, MEDLINE, LILACS, and two trials registries, between 1987 and October 2020. We used 'bloodstream infection' and 'antimicrobial susceptibility tests' as search terms. We had no language or publication status limitations.</p><p><strong>Selection criteria: </strong>Randomized controlled trials (RCTs) comparing rapid antimicrobial susceptibility testing (with a time-to-result of ≤ 8 hours) versus conventional antimicrobial susceptibility testing in people with a BSI caused by any bacteria, as identified by a positive blood culture.</p><p><strong>Data collection and analysis: </strong>Two review authors independently screened references, full-text reports of potentially relevant studies, extracted data from the studies, and assessed risk of bias. Any disagreement was discussed and resolved with a third review author. For mortality, a dichotomous outcome, we extracted the number of events in each arm, and presented a risk ratio (RR) with 95% confidence interval (CI) to compare rapid susceptibility testing to conventional methods. We used Review Manager 5.4 to meta-analyse the data. For other outcomes, which are time-to-event outcomes (time-to-discharge from hospital, time-to-first appropriate antibiotic change), we conducted qualitative narrative synthesis, due to heterogeneity of outcome measures. MAIN RESULTS: We included six trials, with 1638 participants. For rapid antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.10, 95% CI 0.82 to 1.46; 6 RCTs, 1638 participants; low-certainty evidence). In subgroup analysis, for rapid genotypic or molecular antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.02, 95% CI 0.69 to 1.49; 4 RCTs, 1074 participants; low-certainty evidence). For phenotypic rapid susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.37, 95% CI 0.80 to 2.35; 2 RCTs, 564 participants; low-certainty evidence). In qualitative analysis, rapid susceptibility testing may make little or no difference in time-to-discharge (4 RCTs, 1165 participants; low-certainty evidence). In qualitative analysis, rapid genotypic susceptibility testing compared to conventional testing may make little or no difference in time-to-appropriate antibiotic (3 RCTs, 929 participants; low-certainty evidence). In subgroup analysis, rapid phenotypic susceptibility testing compared to conventional testing may improve time-to-appropriate antibiotic (RR -17.29, CI -45.05 to 10.47; 2 RCTs, 564 participants; low-certainty evidence). AUTHORS' CONCLUSIONS: The theoretical benefits of rapid susceptibility testing have not been demonstrated to directly improve mortality, time-to-discharge, or time-to-appropriate antibiotic in these randomized studies. Future large prospective studies should be designed to focus on the most clinically meaningful outcomes, and aim to optimize blood culture pathways.</p>\",\"PeriodicalId\":515753,\"journal\":{\"name\":\"The Cochrane database of systematic reviews\",\"volume\":\" \",\"pages\":\"CD013235\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-05-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/14651858.CD013235.pub2\",\"citationCount\":\"16\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Cochrane database of systematic reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/14651858.CD013235.pub2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cochrane database of systematic reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD013235.pub2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 16
摘要
背景:快速抗微生物药敏试验有望减少获得临床重要血培养结果的时间。这可能使临床医生能够更好地针对个人需求进行治疗,从而改善健康结果(死亡率、住院时间),并减少不必要的广谱抗生素处方;从而降低抗菌素耐药性。目的:评估快速药敏试验与标准药敏试验对血流感染(bsi)的影响。检索方法:为了确定具有选定结果的研究,我们检索了1987年至2020年10月期间的Cochrane传染病组专门登记处、CENTRAL、MEDLINE、LILACS和两个试验登记处。我们使用“血液感染”和“抗菌药物敏感性测试”作为搜索词。我们没有语言或出版状态的限制。选择标准:随机对照试验(rct)比较由任何细菌引起的BSI患者的快速抗菌药物敏感性试验(≤8小时至结果时间)与常规抗菌药物敏感性试验(经血培养阳性确定)。数据收集和分析:两位综述作者独立筛选参考文献和潜在相关研究的全文报告,从研究中提取数据,并评估偏倚风险。任何异议均与第三位综述作者讨论并解决。对于死亡率这一二分类结果,我们提取了每组的事件数,并给出了95%置信区间(CI)的风险比(RR),将快速药敏试验与常规方法进行比较。我们使用Review Manager 5.4对数据进行meta分析。对于其他结果,即事件发生时间(出院时间、首次适当更换抗生素时间),由于结果测量的异质性,我们进行了定性叙事综合。主要结果:我们纳入了6项试验,1638名受试者。与常规方法相比,快速抗菌药物敏感性试验组间死亡率差异很小或没有差异(RR 1.10, 95% CI 0.82 ~ 1.46;6项随机对照试验,1638名受试者;确定性的证据)。在亚组分析中,与常规方法相比,快速基因型或分子抗微生物药敏试验组间死亡率差异很小或没有差异(RR 1.02, 95% CI 0.69 ~ 1.49;4项随机对照试验,1074名受试者;确定性的证据)。与传统方法相比,表型快速敏感性检测组间死亡率差异很小或没有差异(RR 1.37, 95% CI 0.80 ~ 2.35;2项随机对照试验,564名受试者;确定性的证据)。在定性分析中,快速药敏试验对出院时间的影响很小或没有影响(4项随机对照试验,1165名受试者;确定性的证据)。在定性分析中,快速基因型药敏试验与常规试验相比,在获得合适抗生素的时间上可能几乎没有差异(3项随机对照试验,929名受试者;确定性的证据)。在亚组分析中,与常规检测相比,快速表型敏感性检测可缩短患者获得合适抗生素的时间(RR -17.29, CI -45.05 ~ 10.47;2项随机对照试验,564名受试者;确定性的证据)。作者的结论:在这些随机研究中,快速药敏试验的理论益处尚未被证明能直接改善死亡率、出院时间或使用合适抗生素的时间。未来的大型前瞻性研究应侧重于最具临床意义的结果,并旨在优化血培养途径。
Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection.
Background: Rapid antimicrobial susceptibility tests are expected to reduce the time to clinically important results of a blood culture. This might enable clinicians to better target therapy to a person's needs, and thereby, improve health outcomes (mortality, length of hospital stay), and reduce unnecessary prescribing of broad-spectrum antibiotics; thereby reducing antimicrobial resistance rates.
Objectives: To assess the effects of rapid susceptibility testing versus standard susceptibility testing for bloodstream infections (BSIs).
Search methods: To identify studies with selected outcomes, we searched the Cochrane Infectious Diseases Group Specialised Register, CENTRAL, MEDLINE, LILACS, and two trials registries, between 1987 and October 2020. We used 'bloodstream infection' and 'antimicrobial susceptibility tests' as search terms. We had no language or publication status limitations.
Selection criteria: Randomized controlled trials (RCTs) comparing rapid antimicrobial susceptibility testing (with a time-to-result of ≤ 8 hours) versus conventional antimicrobial susceptibility testing in people with a BSI caused by any bacteria, as identified by a positive blood culture.
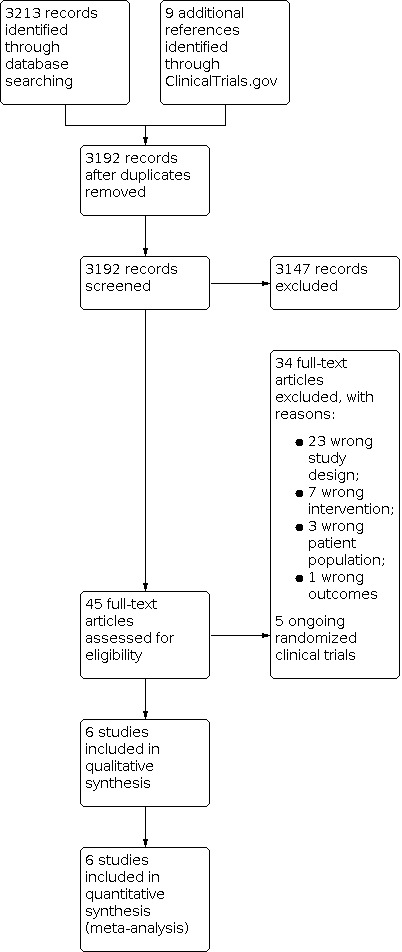
Data collection and analysis: Two review authors independently screened references, full-text reports of potentially relevant studies, extracted data from the studies, and assessed risk of bias. Any disagreement was discussed and resolved with a third review author. For mortality, a dichotomous outcome, we extracted the number of events in each arm, and presented a risk ratio (RR) with 95% confidence interval (CI) to compare rapid susceptibility testing to conventional methods. We used Review Manager 5.4 to meta-analyse the data. For other outcomes, which are time-to-event outcomes (time-to-discharge from hospital, time-to-first appropriate antibiotic change), we conducted qualitative narrative synthesis, due to heterogeneity of outcome measures. MAIN RESULTS: We included six trials, with 1638 participants. For rapid antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.10, 95% CI 0.82 to 1.46; 6 RCTs, 1638 participants; low-certainty evidence). In subgroup analysis, for rapid genotypic or molecular antimicrobial susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.02, 95% CI 0.69 to 1.49; 4 RCTs, 1074 participants; low-certainty evidence). For phenotypic rapid susceptibility testing compared to conventional methods, there was little or no difference in mortality between groups (RR 1.37, 95% CI 0.80 to 2.35; 2 RCTs, 564 participants; low-certainty evidence). In qualitative analysis, rapid susceptibility testing may make little or no difference in time-to-discharge (4 RCTs, 1165 participants; low-certainty evidence). In qualitative analysis, rapid genotypic susceptibility testing compared to conventional testing may make little or no difference in time-to-appropriate antibiotic (3 RCTs, 929 participants; low-certainty evidence). In subgroup analysis, rapid phenotypic susceptibility testing compared to conventional testing may improve time-to-appropriate antibiotic (RR -17.29, CI -45.05 to 10.47; 2 RCTs, 564 participants; low-certainty evidence). AUTHORS' CONCLUSIONS: The theoretical benefits of rapid susceptibility testing have not been demonstrated to directly improve mortality, time-to-discharge, or time-to-appropriate antibiotic in these randomized studies. Future large prospective studies should be designed to focus on the most clinically meaningful outcomes, and aim to optimize blood culture pathways.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


