Chunhu Shi, Jo C Dumville, Nicky Cullum, Sarah Rhodes, Elizabeth McInnes
{"title":"替代反应支持表面(非泡沫和非充气),防止压力溃疡。","authors":"Chunhu Shi, Jo C Dumville, Nicky Cullum, Sarah Rhodes, Elizabeth McInnes","doi":"10.1002/14651858.CD013623.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pressure ulcers (also known as injuries, pressure sores, decubitus ulcers and bed sores) are localised injuries to the skin or underlying soft tissue, or both, caused by unrelieved pressure, shear or friction. Reactive surfaces that are not made of foam or air cells can be used for preventing pressure ulcers.</p><p><strong>Objectives: </strong>To assess the effects of non-foam and non-air-filled reactive beds, mattresses or overlays compared with any other support surface on the incidence of pressure ulcers in any population in any setting.</p><p><strong>Search methods: </strong>In November 2019, we searched the Cochrane Wounds Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL); Ovid MEDLINE (including In-Process & Other Non-Indexed Citations); Ovid Embase and EBSCO CINAHL Plus. We also searched clinical trials registries for ongoing and unpublished studies, and scanned reference lists of relevant included studies as well as reviews, meta-analyses and health technology reports to identify additional studies. There were no restrictions with respect to language, date of publication or study setting.</p><p><strong>Selection criteria: </strong>We included randomised controlled trials that allocated participants of any age to non-foam or non-air-filled reactive beds, overlays or mattresses. Comparators were any beds, overlays or mattresses used.</p><p><strong>Data collection and analysis: </strong>At least two review authors independently assessed studies using predetermined inclusion criteria. We carried out data extraction, 'Risk of bias' assessment using the Cochrane 'Risk of bias' tool, and the certainty of the evidence assessment according to Grading of Recommendations, Assessment, Development and Evaluations methodology. If a non-foam or non-air-filled surface was compared with surfaces that were not clearly specified, then the included study was recorded and described but not considered further in any data analyses.</p><p><strong>Main results: </strong>We included 20 studies (4653 participants) in this review. Most studies were small (median study sample size: 198 participants). The average participant age ranged from 37.2 to 85.4 years (median: 72.5 years). Participants were recruited from a wide range of care settings but were mainly from acute care settings. Almost all studies were conducted in Europe and America. Of the 20 studies, 11 (2826 participants) included surfaces that were not well described and therefore could not be fully classified. We synthesised data for the following 12 comparisons: (1) reactive water surfaces versus alternating pressure (active) air surfaces (three studies with 414 participants), (2) reactive water surfaces versus foam surfaces (one study with 117 participants), (3) reactive water surfaces versus reactive air surfaces (one study with 37 participants), (4) reactive water surfaces versus reactive fibre surfaces (one study with 87 participants), (5) reactive fibre surfaces versus alternating pressure (active) air surfaces (four studies with 384 participants), (6) reactive fibre surfaces versus foam surfaces (two studies with 228 participants), (7) reactive gel surfaces on operating tables followed by foam surfaces on ward beds versus alternating pressure (active) air surfaces on operating tables and subsequently on ward beds (two studies with 415 participants), (8) reactive gel surfaces versus reactive air surfaces (one study with 74 participants), (9) reactive gel surfaces versus foam surfaces (one study with 135 participants), (10) reactive gel surfaces versus reactive gel surfaces (one study with 113 participants), (11) reactive foam and gel surfaces versus reactive gel surfaces (one study with 166 participants) and (12) reactive foam and gel surfaces versus foam surfaces (one study with 91 participants). Of the 20 studies, 16 (80%) presented findings which were considered to be at high overall risk of bias.</p><p><strong>Primary outcome: </strong>Pressure ulcer incidence We did not find analysable data for two comparisons: reactive water surfaces versus foam surfaces, and reactive water surfaces versus reactive fibre surfaces. Reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds (14/205 (6.8%)) may increase the proportion of people developing a new pressure ulcer compared with alternating pressure (active) air surfaces applied on both operating tables and hospital beds (3/210 (1.4%) (risk ratio 4.53, 95% confidence interval 1.31 to 15.65; 2 studies, 415 participants; I<sup>2</sup> = 0%; low-certainty evidence). For all other comparisons, it is uncertain whether there is a difference in the proportion of participants developing new pressure ulcers as all data were of very low certainty. Included studies did not report time to pressure ulcer incidence for any comparison in this review. Secondary outcomes Support-surface-associated patient comfort: the included studies provide data on this outcome for one comparison. It is uncertain if there is a difference in patient comfort between alternating pressure (active) air surfaces and reactive fibre surfaces (one study with 187 participants; very low-certainty evidence). All reported adverse events: there is evidence on this outcome for one comparison. It is uncertain if there is a difference in adverse events between reactive gel surfaces followed by foam surfaces and alternating pressure (active) air surfaces applied on both operating tables and hospital beds (one study with 198 participants; very low-certainty evidence). We did not find any health-related quality of life or cost-effectiveness evidence for any comparison in this review.</p><p><strong>Authors' conclusions: </strong>Current evidence is generally uncertain about the differences between non-foam and non-air-filled reactive surfaces and other surfaces in terms of pressure ulcer incidence, patient comfort, adverse effects, health-related quality of life and cost-effectiveness. Reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds may increase the risk of having new pressure ulcers compared with alternating pressure (active) air surfaces applied on both operating tables and hospital beds. Future research in this area should consider evaluation of the most important support surfaces from the perspective of decision-makers. Time-to-event outcomes, careful assessment of adverse events and trial-level cost-effectiveness evaluation should be considered in future studies. Trials should be designed to minimise the risk of detection bias; for example, by using digital photography and adjudicators of the photographs being blinded to group allocation. Further review using network meta-analysis will add to the findings reported here.</p>","PeriodicalId":515753,"journal":{"name":"The Cochrane database of systematic reviews","volume":" ","pages":"CD013623"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/14651858.CD013623.pub2","citationCount":"6","resultStr":"{\"title\":\"Alternative reactive support surfaces (non-foam and non-air-filled) for preventing pressure ulcers.\",\"authors\":\"Chunhu Shi, Jo C Dumville, Nicky Cullum, Sarah Rhodes, Elizabeth McInnes\",\"doi\":\"10.1002/14651858.CD013623.pub2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pressure ulcers (also known as injuries, pressure sores, decubitus ulcers and bed sores) are localised injuries to the skin or underlying soft tissue, or both, caused by unrelieved pressure, shear or friction. Reactive surfaces that are not made of foam or air cells can be used for preventing pressure ulcers.</p><p><strong>Objectives: </strong>To assess the effects of non-foam and non-air-filled reactive beds, mattresses or overlays compared with any other support surface on the incidence of pressure ulcers in any population in any setting.</p><p><strong>Search methods: </strong>In November 2019, we searched the Cochrane Wounds Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL); Ovid MEDLINE (including In-Process & Other Non-Indexed Citations); Ovid Embase and EBSCO CINAHL Plus. We also searched clinical trials registries for ongoing and unpublished studies, and scanned reference lists of relevant included studies as well as reviews, meta-analyses and health technology reports to identify additional studies. There were no restrictions with respect to language, date of publication or study setting.</p><p><strong>Selection criteria: </strong>We included randomised controlled trials that allocated participants of any age to non-foam or non-air-filled reactive beds, overlays or mattresses. Comparators were any beds, overlays or mattresses used.</p><p><strong>Data collection and analysis: </strong>At least two review authors independently assessed studies using predetermined inclusion criteria. We carried out data extraction, 'Risk of bias' assessment using the Cochrane 'Risk of bias' tool, and the certainty of the evidence assessment according to Grading of Recommendations, Assessment, Development and Evaluations methodology. If a non-foam or non-air-filled surface was compared with surfaces that were not clearly specified, then the included study was recorded and described but not considered further in any data analyses.</p><p><strong>Main results: </strong>We included 20 studies (4653 participants) in this review. Most studies were small (median study sample size: 198 participants). The average participant age ranged from 37.2 to 85.4 years (median: 72.5 years). Participants were recruited from a wide range of care settings but were mainly from acute care settings. Almost all studies were conducted in Europe and America. Of the 20 studies, 11 (2826 participants) included surfaces that were not well described and therefore could not be fully classified. We synthesised data for the following 12 comparisons: (1) reactive water surfaces versus alternating pressure (active) air surfaces (three studies with 414 participants), (2) reactive water surfaces versus foam surfaces (one study with 117 participants), (3) reactive water surfaces versus reactive air surfaces (one study with 37 participants), (4) reactive water surfaces versus reactive fibre surfaces (one study with 87 participants), (5) reactive fibre surfaces versus alternating pressure (active) air surfaces (four studies with 384 participants), (6) reactive fibre surfaces versus foam surfaces (two studies with 228 participants), (7) reactive gel surfaces on operating tables followed by foam surfaces on ward beds versus alternating pressure (active) air surfaces on operating tables and subsequently on ward beds (two studies with 415 participants), (8) reactive gel surfaces versus reactive air surfaces (one study with 74 participants), (9) reactive gel surfaces versus foam surfaces (one study with 135 participants), (10) reactive gel surfaces versus reactive gel surfaces (one study with 113 participants), (11) reactive foam and gel surfaces versus reactive gel surfaces (one study with 166 participants) and (12) reactive foam and gel surfaces versus foam surfaces (one study with 91 participants). Of the 20 studies, 16 (80%) presented findings which were considered to be at high overall risk of bias.</p><p><strong>Primary outcome: </strong>Pressure ulcer incidence We did not find analysable data for two comparisons: reactive water surfaces versus foam surfaces, and reactive water surfaces versus reactive fibre surfaces. Reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds (14/205 (6.8%)) may increase the proportion of people developing a new pressure ulcer compared with alternating pressure (active) air surfaces applied on both operating tables and hospital beds (3/210 (1.4%) (risk ratio 4.53, 95% confidence interval 1.31 to 15.65; 2 studies, 415 participants; I<sup>2</sup> = 0%; low-certainty evidence). For all other comparisons, it is uncertain whether there is a difference in the proportion of participants developing new pressure ulcers as all data were of very low certainty. Included studies did not report time to pressure ulcer incidence for any comparison in this review. Secondary outcomes Support-surface-associated patient comfort: the included studies provide data on this outcome for one comparison. It is uncertain if there is a difference in patient comfort between alternating pressure (active) air surfaces and reactive fibre surfaces (one study with 187 participants; very low-certainty evidence). All reported adverse events: there is evidence on this outcome for one comparison. It is uncertain if there is a difference in adverse events between reactive gel surfaces followed by foam surfaces and alternating pressure (active) air surfaces applied on both operating tables and hospital beds (one study with 198 participants; very low-certainty evidence). We did not find any health-related quality of life or cost-effectiveness evidence for any comparison in this review.</p><p><strong>Authors' conclusions: </strong>Current evidence is generally uncertain about the differences between non-foam and non-air-filled reactive surfaces and other surfaces in terms of pressure ulcer incidence, patient comfort, adverse effects, health-related quality of life and cost-effectiveness. Reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds may increase the risk of having new pressure ulcers compared with alternating pressure (active) air surfaces applied on both operating tables and hospital beds. Future research in this area should consider evaluation of the most important support surfaces from the perspective of decision-makers. Time-to-event outcomes, careful assessment of adverse events and trial-level cost-effectiveness evaluation should be considered in future studies. Trials should be designed to minimise the risk of detection bias; for example, by using digital photography and adjudicators of the photographs being blinded to group allocation. Further review using network meta-analysis will add to the findings reported here.</p>\",\"PeriodicalId\":515753,\"journal\":{\"name\":\"The Cochrane database of systematic reviews\",\"volume\":\" \",\"pages\":\"CD013623\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/14651858.CD013623.pub2\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Cochrane database of systematic reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/14651858.CD013623.pub2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cochrane database of systematic reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD013623.pub2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Alternative reactive support surfaces (non-foam and non-air-filled) for preventing pressure ulcers.
Background: Pressure ulcers (also known as injuries, pressure sores, decubitus ulcers and bed sores) are localised injuries to the skin or underlying soft tissue, or both, caused by unrelieved pressure, shear or friction. Reactive surfaces that are not made of foam or air cells can be used for preventing pressure ulcers.
Objectives: To assess the effects of non-foam and non-air-filled reactive beds, mattresses or overlays compared with any other support surface on the incidence of pressure ulcers in any population in any setting.
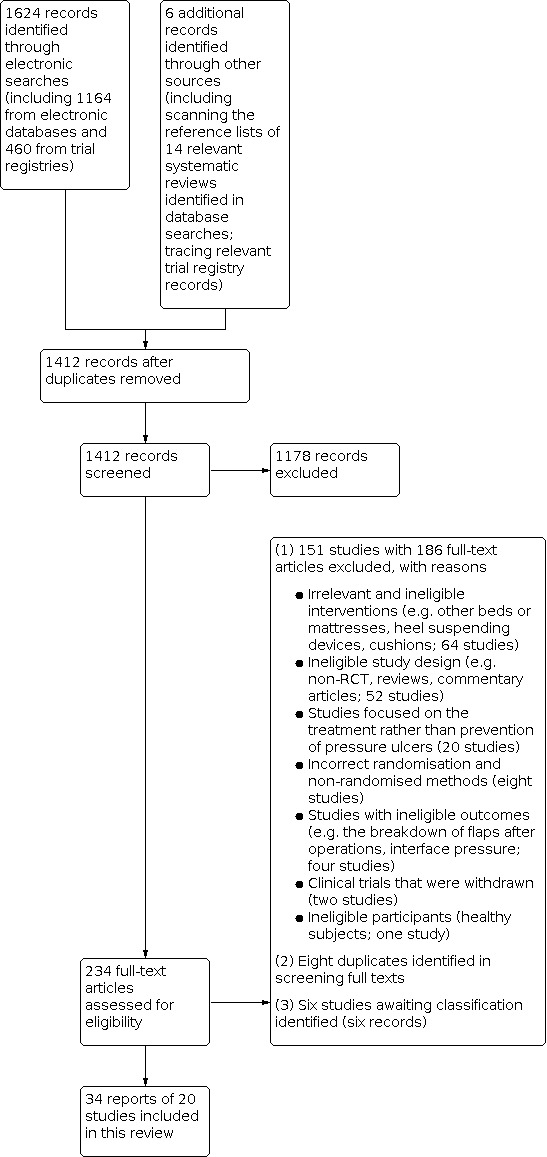
Search methods: In November 2019, we searched the Cochrane Wounds Specialised Register; the Cochrane Central Register of Controlled Trials (CENTRAL); Ovid MEDLINE (including In-Process & Other Non-Indexed Citations); Ovid Embase and EBSCO CINAHL Plus. We also searched clinical trials registries for ongoing and unpublished studies, and scanned reference lists of relevant included studies as well as reviews, meta-analyses and health technology reports to identify additional studies. There were no restrictions with respect to language, date of publication or study setting.
Selection criteria: We included randomised controlled trials that allocated participants of any age to non-foam or non-air-filled reactive beds, overlays or mattresses. Comparators were any beds, overlays or mattresses used.
Data collection and analysis: At least two review authors independently assessed studies using predetermined inclusion criteria. We carried out data extraction, 'Risk of bias' assessment using the Cochrane 'Risk of bias' tool, and the certainty of the evidence assessment according to Grading of Recommendations, Assessment, Development and Evaluations methodology. If a non-foam or non-air-filled surface was compared with surfaces that were not clearly specified, then the included study was recorded and described but not considered further in any data analyses.
Main results: We included 20 studies (4653 participants) in this review. Most studies were small (median study sample size: 198 participants). The average participant age ranged from 37.2 to 85.4 years (median: 72.5 years). Participants were recruited from a wide range of care settings but were mainly from acute care settings. Almost all studies were conducted in Europe and America. Of the 20 studies, 11 (2826 participants) included surfaces that were not well described and therefore could not be fully classified. We synthesised data for the following 12 comparisons: (1) reactive water surfaces versus alternating pressure (active) air surfaces (three studies with 414 participants), (2) reactive water surfaces versus foam surfaces (one study with 117 participants), (3) reactive water surfaces versus reactive air surfaces (one study with 37 participants), (4) reactive water surfaces versus reactive fibre surfaces (one study with 87 participants), (5) reactive fibre surfaces versus alternating pressure (active) air surfaces (four studies with 384 participants), (6) reactive fibre surfaces versus foam surfaces (two studies with 228 participants), (7) reactive gel surfaces on operating tables followed by foam surfaces on ward beds versus alternating pressure (active) air surfaces on operating tables and subsequently on ward beds (two studies with 415 participants), (8) reactive gel surfaces versus reactive air surfaces (one study with 74 participants), (9) reactive gel surfaces versus foam surfaces (one study with 135 participants), (10) reactive gel surfaces versus reactive gel surfaces (one study with 113 participants), (11) reactive foam and gel surfaces versus reactive gel surfaces (one study with 166 participants) and (12) reactive foam and gel surfaces versus foam surfaces (one study with 91 participants). Of the 20 studies, 16 (80%) presented findings which were considered to be at high overall risk of bias.
Primary outcome: Pressure ulcer incidence We did not find analysable data for two comparisons: reactive water surfaces versus foam surfaces, and reactive water surfaces versus reactive fibre surfaces. Reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds (14/205 (6.8%)) may increase the proportion of people developing a new pressure ulcer compared with alternating pressure (active) air surfaces applied on both operating tables and hospital beds (3/210 (1.4%) (risk ratio 4.53, 95% confidence interval 1.31 to 15.65; 2 studies, 415 participants; I2 = 0%; low-certainty evidence). For all other comparisons, it is uncertain whether there is a difference in the proportion of participants developing new pressure ulcers as all data were of very low certainty. Included studies did not report time to pressure ulcer incidence for any comparison in this review. Secondary outcomes Support-surface-associated patient comfort: the included studies provide data on this outcome for one comparison. It is uncertain if there is a difference in patient comfort between alternating pressure (active) air surfaces and reactive fibre surfaces (one study with 187 participants; very low-certainty evidence). All reported adverse events: there is evidence on this outcome for one comparison. It is uncertain if there is a difference in adverse events between reactive gel surfaces followed by foam surfaces and alternating pressure (active) air surfaces applied on both operating tables and hospital beds (one study with 198 participants; very low-certainty evidence). We did not find any health-related quality of life or cost-effectiveness evidence for any comparison in this review.
Authors' conclusions: Current evidence is generally uncertain about the differences between non-foam and non-air-filled reactive surfaces and other surfaces in terms of pressure ulcer incidence, patient comfort, adverse effects, health-related quality of life and cost-effectiveness. Reactive gel surfaces used on operating tables followed by foam surfaces applied on hospital beds may increase the risk of having new pressure ulcers compared with alternating pressure (active) air surfaces applied on both operating tables and hospital beds. Future research in this area should consider evaluation of the most important support surfaces from the perspective of decision-makers. Time-to-event outcomes, careful assessment of adverse events and trial-level cost-effectiveness evaluation should be considered in future studies. Trials should be designed to minimise the risk of detection bias; for example, by using digital photography and adjudicators of the photographs being blinded to group allocation. Further review using network meta-analysis will add to the findings reported here.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


