Edward J M Monk, Katharine Abba, Lakshmi N Ranganathan
{"title":"神经囊虫病患者的驱虫药。","authors":"Edward J M Monk, Katharine Abba, Lakshmi N Ranganathan","doi":"10.1002/14651858.CD000215.pub5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neurocysticercosis is a parasitic infection of the central nervous system by the larval stage of the pork tapeworm and is a common cause of seizures and epilepsy in endemic areas. Anthelmintics (albendazole or praziquantel) may be given alongside supportive treatment (antiepileptics/analgesia) with the aim of killing these larvae (cysticerci), with or without corticosteroid treatment. However, there are potential adverse effects of these drugs, and the cysticerci may eventually die without directed anthelminthic treatment.</p><p><strong>Objectives: </strong>To assess the effects of anthelmintics on people with neurocysticercosis.</p><p><strong>Search methods: </strong>We searched the Cochrane Infectious Diseases Group Specialized Register, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, LILACS, the WHO ICTRP, and ClinicalTrials.gov, up to 21 October 2020.</p><p><strong>Selection criteria: </strong>Randomized controlled trials comparing anthelmintics and supportive treatment (+/- corticosteroids) with supportive treatment alone (+/- corticosteroids) for people with neurocysticercosis.</p><p><strong>Data collection and analysis: </strong>Two review authors independently screened the title and abstract of all articles identified by the search. We obtained full-text articles to confirm the eligibility of all studies that passed screening. One review author extracted data, which a second review author checked. Two review authors assessed the risk of bias of each trial and performed GRADE assessments. In cases of disagreement at consensus discussion stage between review authors, we consulted a third review author. We calculated risk ratios (RR) for dichotomous variables, with 95% confidence intervals (CIs) for pooled data from studies with similar interventions and outcomes.</p><p><strong>Main results: </strong>We included 16 studies in the review. Only two studies investigated praziquantel and did not report data in a format that could contribute to meta-analysis. Most results in this review are therefore applicable to albendazole versus placebo or no anthelmintic. The aggregate analysis across all participants with neurocysticercosis did not demonstrate a difference between groups in seizure recurrence, but heterogeneity was marked (RR 0.94, 95% CI 0.78 to 1.14; 10 trials, 1054 participants; I<sup>2</sup> = 67%; low-certainty evidence). When stratified by participants with a single cyst or multiple cysts, pooled analysis suggests that albendazole probably improves seizure recurrence for participants with a single cyst (RR 0.61, 95% CI 0.4 to 0.91; 5 trials, 396 participants; moderate-certainty evidence). All studies contributing to this analysis recruited participants with non-viable, intraparenchymal cysts only, and most participants were children. We are uncertain whether or not albendazole reduces seizure recurrence in participants with multiple cysts, as the certainty of the evidence is very low, although the direction of effect is towards albendazole causing harm (RR 2.05, 95% CI 1.28 to 3.31; 2 trials, 321 participants; very low-certainty evidence). This analysis included a large study containing a highly heterogeneous population that received an assessment of unclear risk for multiple 'Risk of bias' domains. Regarding radiological outcomes, albendazole probably slightly improves the complete radiological clearance of lesions (RR 1.22, 95% CI 1.07 to 1.39; 13 trials, 1324 participants; moderate-certainty evidence) and the evolution of cysts (RR 1.27, 95% CI 1.10 to 1.47; 6 trials, 434 participants; moderate-certainty evidence). More adverse events appeared to be observed in participants treated with either albendazole or praziquantel compared to those receiving placebo or no anthelmintic. The most commonly reported side effects were headache, abdominal pain, and nausea/vomiting.</p><p><strong>Authors' conclusions: </strong>For participants with a single cyst, there was less seizure recurrence in the albendazole group compared to the placebo/no anthelmintic group. The studies contributing to this evidence only recruited participants with a non-viable intraparenchymal cyst. We are uncertain whether albendazole reduces seizure recurrence for participants with multiple cysts. We also found that albendazole probably increases radiological clearance and evolution of lesions. There were very few studies reporting praziquantel outcomes, and these findings apply to albendazole only.</p>","PeriodicalId":515753,"journal":{"name":"The Cochrane database of systematic reviews","volume":" ","pages":"CD000215"},"PeriodicalIF":0.0000,"publicationDate":"2021-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/14651858.CD000215.pub5","citationCount":"2","resultStr":"{\"title\":\"Anthelmintics for people with neurocysticercosis.\",\"authors\":\"Edward J M Monk, Katharine Abba, Lakshmi N Ranganathan\",\"doi\":\"10.1002/14651858.CD000215.pub5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neurocysticercosis is a parasitic infection of the central nervous system by the larval stage of the pork tapeworm and is a common cause of seizures and epilepsy in endemic areas. Anthelmintics (albendazole or praziquantel) may be given alongside supportive treatment (antiepileptics/analgesia) with the aim of killing these larvae (cysticerci), with or without corticosteroid treatment. However, there are potential adverse effects of these drugs, and the cysticerci may eventually die without directed anthelminthic treatment.</p><p><strong>Objectives: </strong>To assess the effects of anthelmintics on people with neurocysticercosis.</p><p><strong>Search methods: </strong>We searched the Cochrane Infectious Diseases Group Specialized Register, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, LILACS, the WHO ICTRP, and ClinicalTrials.gov, up to 21 October 2020.</p><p><strong>Selection criteria: </strong>Randomized controlled trials comparing anthelmintics and supportive treatment (+/- corticosteroids) with supportive treatment alone (+/- corticosteroids) for people with neurocysticercosis.</p><p><strong>Data collection and analysis: </strong>Two review authors independently screened the title and abstract of all articles identified by the search. We obtained full-text articles to confirm the eligibility of all studies that passed screening. One review author extracted data, which a second review author checked. Two review authors assessed the risk of bias of each trial and performed GRADE assessments. In cases of disagreement at consensus discussion stage between review authors, we consulted a third review author. We calculated risk ratios (RR) for dichotomous variables, with 95% confidence intervals (CIs) for pooled data from studies with similar interventions and outcomes.</p><p><strong>Main results: </strong>We included 16 studies in the review. Only two studies investigated praziquantel and did not report data in a format that could contribute to meta-analysis. Most results in this review are therefore applicable to albendazole versus placebo or no anthelmintic. The aggregate analysis across all participants with neurocysticercosis did not demonstrate a difference between groups in seizure recurrence, but heterogeneity was marked (RR 0.94, 95% CI 0.78 to 1.14; 10 trials, 1054 participants; I<sup>2</sup> = 67%; low-certainty evidence). When stratified by participants with a single cyst or multiple cysts, pooled analysis suggests that albendazole probably improves seizure recurrence for participants with a single cyst (RR 0.61, 95% CI 0.4 to 0.91; 5 trials, 396 participants; moderate-certainty evidence). All studies contributing to this analysis recruited participants with non-viable, intraparenchymal cysts only, and most participants were children. We are uncertain whether or not albendazole reduces seizure recurrence in participants with multiple cysts, as the certainty of the evidence is very low, although the direction of effect is towards albendazole causing harm (RR 2.05, 95% CI 1.28 to 3.31; 2 trials, 321 participants; very low-certainty evidence). This analysis included a large study containing a highly heterogeneous population that received an assessment of unclear risk for multiple 'Risk of bias' domains. Regarding radiological outcomes, albendazole probably slightly improves the complete radiological clearance of lesions (RR 1.22, 95% CI 1.07 to 1.39; 13 trials, 1324 participants; moderate-certainty evidence) and the evolution of cysts (RR 1.27, 95% CI 1.10 to 1.47; 6 trials, 434 participants; moderate-certainty evidence). More adverse events appeared to be observed in participants treated with either albendazole or praziquantel compared to those receiving placebo or no anthelmintic. The most commonly reported side effects were headache, abdominal pain, and nausea/vomiting.</p><p><strong>Authors' conclusions: </strong>For participants with a single cyst, there was less seizure recurrence in the albendazole group compared to the placebo/no anthelmintic group. The studies contributing to this evidence only recruited participants with a non-viable intraparenchymal cyst. We are uncertain whether albendazole reduces seizure recurrence for participants with multiple cysts. We also found that albendazole probably increases radiological clearance and evolution of lesions. There were very few studies reporting praziquantel outcomes, and these findings apply to albendazole only.</p>\",\"PeriodicalId\":515753,\"journal\":{\"name\":\"The Cochrane database of systematic reviews\",\"volume\":\" \",\"pages\":\"CD000215\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/14651858.CD000215.pub5\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Cochrane database of systematic reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/14651858.CD000215.pub5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cochrane database of systematic reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD000215.pub5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
摘要
背景:神经囊虫病是一种由猪绦虫幼虫期引起的中枢神经系统寄生虫感染,是流行地区癫痫发作的常见病因。抗虫药(阿苯达唑或吡喹酮)可与支持治疗(抗癫痫药/镇痛药)一起给予,目的是杀死这些幼虫(囊虫),有或没有皮质类固醇治疗。然而,这些药物有潜在的不良反应,并且囊虫最终可能在没有直接驱虫治疗的情况下死亡。目的:评价驱虫药对神经囊虫病患者的治疗效果。检索方法:我们检索了截至2020年10月21日的Cochrane传染病组专业注册库、Cochrane中央对照试验注册库(Central)、MEDLINE、Embase、LILACS、WHO ICTRP和ClinicalTrials.gov。选择标准:随机对照试验比较驱虫药和支持治疗(+/-皮质类固醇)与单独支持治疗(+/-皮质类固醇)对神经囊虫病患者的疗效。数据收集和分析:两位综述作者独立筛选检索到的所有文章的标题和摘要。我们获得了全文文章来确认所有通过筛选的研究的合格性。一位综述作者提取数据,另一位综述作者检查数据。两位综述作者评估了每个试验的偏倚风险,并进行了GRADE评估。如果在综述作者之间的共识讨论阶段存在分歧,我们会咨询第三位综述作者。我们计算了二分类变量的风险比(RR),对具有相似干预措施和结果的研究汇总数据采用95%置信区间(ci)。主要结果:我们纳入了16项研究。只有两项研究调查了吡喹酮,但没有以一种可以用于荟萃分析的格式报告数据。因此,本综述中的大多数结果适用于阿苯达唑与安慰剂或无驱虫药的比较。对所有神经囊虫病患者的综合分析未显示两组之间癫痫复发的差异,但异质性显著(RR 0.94, 95% CI 0.78 ~ 1.14;10项试验,1054名受试者;i2 = 67%;确定性的证据)。当按单个囊肿或多个囊肿的参与者分层时,汇总分析表明阿苯达唑可能改善单个囊肿参与者的癫痫复发(RR 0.61, 95% CI 0.4至0.91;5项试验,396名受试者;moderate-certainty证据)。所有有助于这一分析的研究只招募了无活力的肺实质内囊肿的参与者,并且大多数参与者是儿童。我们不确定阿苯达唑是否能减少多发性囊肿患者的癫痫复发,因为证据的确定性非常低,尽管效果的方向是阿苯达唑会造成伤害(RR 2.05, 95% CI 1.28至3.31;2项试验,321名受试者;非常低确定性证据)。该分析包括一项包含高度异质人群的大型研究,该研究接受了多个“偏倚风险”域的不明确风险评估。关于放射学结果,阿苯达唑可能略微改善病变的完全放射清除率(RR 1.22, 95% CI 1.07至1.39;13项试验,1324名受试者;中度确定性证据)和囊肿的演变(RR 1.27, 95% CI 1.10 ~ 1.47;6项试验,434名受试者;moderate-certainty证据)。服用阿苯达唑或吡喹酮的受试者与服用安慰剂或不服用驱虫药的受试者相比,出现了更多的不良事件。最常见的副作用是头痛、腹痛和恶心/呕吐。作者的结论:对于单个囊肿的参与者,阿苯达唑组与安慰剂/无驱虫药组相比,癫痫复发率更低。提供这一证据的研究只招募了有不可存活的实质内囊肿的参与者。我们不确定阿苯达唑是否能减少多发性囊肿患者的癫痫复发。我们还发现阿苯达唑可能增加放射清除率和病变的发展。很少有研究报告吡喹酮的结果,这些发现仅适用于阿苯达唑。
Background: Neurocysticercosis is a parasitic infection of the central nervous system by the larval stage of the pork tapeworm and is a common cause of seizures and epilepsy in endemic areas. Anthelmintics (albendazole or praziquantel) may be given alongside supportive treatment (antiepileptics/analgesia) with the aim of killing these larvae (cysticerci), with or without corticosteroid treatment. However, there are potential adverse effects of these drugs, and the cysticerci may eventually die without directed anthelminthic treatment.
Objectives: To assess the effects of anthelmintics on people with neurocysticercosis.
Search methods: We searched the Cochrane Infectious Diseases Group Specialized Register, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, LILACS, the WHO ICTRP, and ClinicalTrials.gov, up to 21 October 2020.
Selection criteria: Randomized controlled trials comparing anthelmintics and supportive treatment (+/- corticosteroids) with supportive treatment alone (+/- corticosteroids) for people with neurocysticercosis.
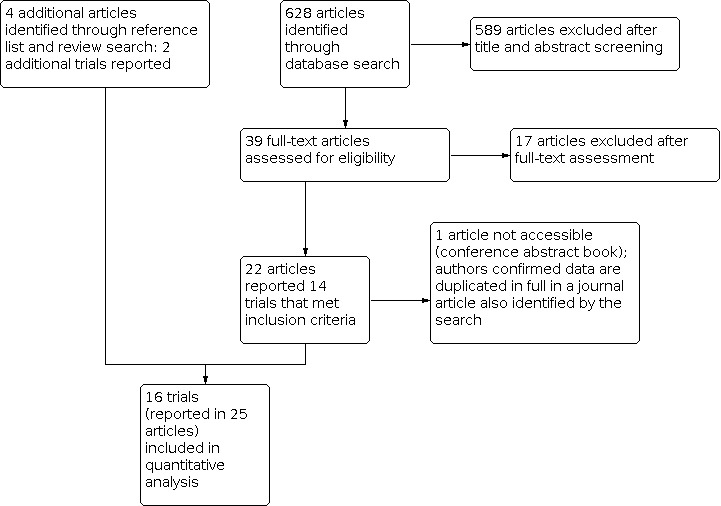
Data collection and analysis: Two review authors independently screened the title and abstract of all articles identified by the search. We obtained full-text articles to confirm the eligibility of all studies that passed screening. One review author extracted data, which a second review author checked. Two review authors assessed the risk of bias of each trial and performed GRADE assessments. In cases of disagreement at consensus discussion stage between review authors, we consulted a third review author. We calculated risk ratios (RR) for dichotomous variables, with 95% confidence intervals (CIs) for pooled data from studies with similar interventions and outcomes.
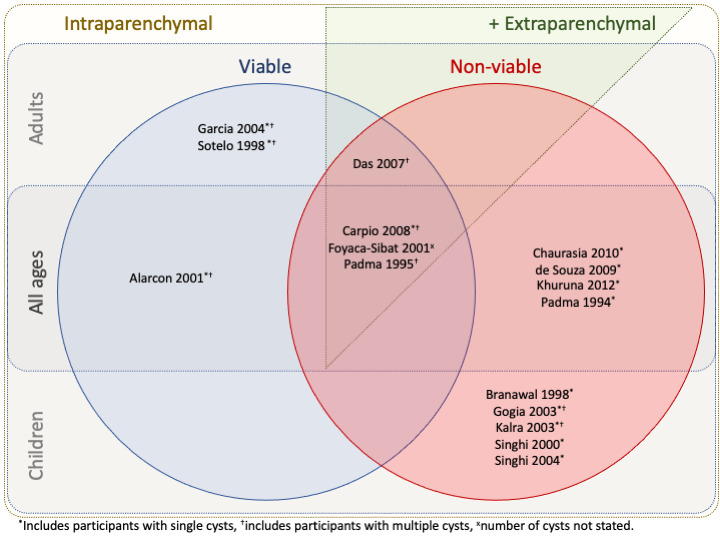
Main results: We included 16 studies in the review. Only two studies investigated praziquantel and did not report data in a format that could contribute to meta-analysis. Most results in this review are therefore applicable to albendazole versus placebo or no anthelmintic. The aggregate analysis across all participants with neurocysticercosis did not demonstrate a difference between groups in seizure recurrence, but heterogeneity was marked (RR 0.94, 95% CI 0.78 to 1.14; 10 trials, 1054 participants; I2 = 67%; low-certainty evidence). When stratified by participants with a single cyst or multiple cysts, pooled analysis suggests that albendazole probably improves seizure recurrence for participants with a single cyst (RR 0.61, 95% CI 0.4 to 0.91; 5 trials, 396 participants; moderate-certainty evidence). All studies contributing to this analysis recruited participants with non-viable, intraparenchymal cysts only, and most participants were children. We are uncertain whether or not albendazole reduces seizure recurrence in participants with multiple cysts, as the certainty of the evidence is very low, although the direction of effect is towards albendazole causing harm (RR 2.05, 95% CI 1.28 to 3.31; 2 trials, 321 participants; very low-certainty evidence). This analysis included a large study containing a highly heterogeneous population that received an assessment of unclear risk for multiple 'Risk of bias' domains. Regarding radiological outcomes, albendazole probably slightly improves the complete radiological clearance of lesions (RR 1.22, 95% CI 1.07 to 1.39; 13 trials, 1324 participants; moderate-certainty evidence) and the evolution of cysts (RR 1.27, 95% CI 1.10 to 1.47; 6 trials, 434 participants; moderate-certainty evidence). More adverse events appeared to be observed in participants treated with either albendazole or praziquantel compared to those receiving placebo or no anthelmintic. The most commonly reported side effects were headache, abdominal pain, and nausea/vomiting.
Authors' conclusions: For participants with a single cyst, there was less seizure recurrence in the albendazole group compared to the placebo/no anthelmintic group. The studies contributing to this evidence only recruited participants with a non-viable intraparenchymal cyst. We are uncertain whether albendazole reduces seizure recurrence for participants with multiple cysts. We also found that albendazole probably increases radiological clearance and evolution of lesions. There were very few studies reporting praziquantel outcomes, and these findings apply to albendazole only.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


