Alvaro Sanchez, Susana Pablo, Arturo Garcia-Alvarez, Silvia Dominguez, Gonzalo Grandes
{"title":"采用协同建模实施策略(PVS-PREDIAPS策略)优化初级保健中2型糖尿病预防的两种程序的有效性:PREDIAPS集群随机混合II型实施试验","authors":"Alvaro Sanchez, Susana Pablo, Arturo Garcia-Alvarez, Silvia Dominguez, Gonzalo Grandes","doi":"10.1186/s13012-021-01127-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The most efficient procedures to engage and guide healthcare professionals in collaborative processes that seek to optimize practice are unknown. The PREDIAPS project aims to assess the effectiveness and feasibility of different procedures to perform a facilitated interprofessional collaborative process to optimize type 2 diabetes prevention in routine primary care.</p><p><strong>Methods: </strong>A type II hybrid cluster randomized implementation trial was conducted in nine primary care centers of the Basque Health Service. All centers received training on effective healthy lifestyle promotion. Headed by a local leader and an external facilitator, centers conducted a collaborative structured process-the PVS-PREDIAPS implementation strategy-to adapt the intervention and its implementation to their specific context. The centers were randomly allocated to one of two groups: one group applied the implementation strategy globally, promoting the cooperation of all health professionals from the beginning, and the other performed it sequentially, centered first on nurses, who later sought the pragmatic cooperation of physicians. The following patients were eligible for inclusion: all those aged ≥ 30 years old with at least one known cardiovascular risk factor and an impaired fasting glucose level (≥ 110-125 mg/dl) but without diabetes who attended centers during the study period. The main outcome measures concerned changes in type 2 diabetes prevention practice indicators after 12 months.</p><p><strong>Results: </strong>After 12 months, 3273 eligible patients at risk of type 2 diabetes had attended their family physician at least once, and of these, 490 (15%) have been addressed by assessing their healthy lifestyles in both comparison groups. The proportion of at-risk patients receiving a personalized prescription of lifestyle change was slightly higher (8.6%; range 13.5-5.9% vs 6.8%; range 7.2-5.8%) and 2.3 times more likely (95% CI for adjusted hazard ratio, 1.38-3.94) in the sequential than in the global centers, after 8 months of the intervention program implementation period. The probability of meeting the recommended levels of physical activity and fruit and vegetable intake were four- and threefold higher after the prescription of lifestyle change than only assessment and provision of advice. The procedure of engagement in and execution of the implementation strategy does not modify the effect of prescribing healthy habits (p interaction component of intervention by group, p > 0.05).</p><p><strong>Discussion: </strong>Our results show that the PVS-PREDIAPS implementation strategy manages to integrate interventions with proven efficacy in the prevention of type 2 diabetes in clinical practice in primary care. Further, they suggest that implementation outcomes were somewhat better with a sequential facilitated collaborative process focused on enhancing the autonomy and responsibility of nurses who subsequently seek a pragmatic cooperation of GPs.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov identifier: NCT03254979 . Registered 16 August 2017-retrospectively registered.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"58"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13012-021-01127-x","citationCount":"3","resultStr":"{\"title\":\"Effectiveness of two procedures for deploying a facilitated collaborative modeling implementation strategy-the PVS-PREDIAPS strategy-to optimize type 2 diabetes prevention in primary care: the PREDIAPS cluster randomized hybrid type II implementation trial.\",\"authors\":\"Alvaro Sanchez, Susana Pablo, Arturo Garcia-Alvarez, Silvia Dominguez, Gonzalo Grandes\",\"doi\":\"10.1186/s13012-021-01127-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The most efficient procedures to engage and guide healthcare professionals in collaborative processes that seek to optimize practice are unknown. The PREDIAPS project aims to assess the effectiveness and feasibility of different procedures to perform a facilitated interprofessional collaborative process to optimize type 2 diabetes prevention in routine primary care.</p><p><strong>Methods: </strong>A type II hybrid cluster randomized implementation trial was conducted in nine primary care centers of the Basque Health Service. All centers received training on effective healthy lifestyle promotion. Headed by a local leader and an external facilitator, centers conducted a collaborative structured process-the PVS-PREDIAPS implementation strategy-to adapt the intervention and its implementation to their specific context. The centers were randomly allocated to one of two groups: one group applied the implementation strategy globally, promoting the cooperation of all health professionals from the beginning, and the other performed it sequentially, centered first on nurses, who later sought the pragmatic cooperation of physicians. The following patients were eligible for inclusion: all those aged ≥ 30 years old with at least one known cardiovascular risk factor and an impaired fasting glucose level (≥ 110-125 mg/dl) but without diabetes who attended centers during the study period. The main outcome measures concerned changes in type 2 diabetes prevention practice indicators after 12 months.</p><p><strong>Results: </strong>After 12 months, 3273 eligible patients at risk of type 2 diabetes had attended their family physician at least once, and of these, 490 (15%) have been addressed by assessing their healthy lifestyles in both comparison groups. The proportion of at-risk patients receiving a personalized prescription of lifestyle change was slightly higher (8.6%; range 13.5-5.9% vs 6.8%; range 7.2-5.8%) and 2.3 times more likely (95% CI for adjusted hazard ratio, 1.38-3.94) in the sequential than in the global centers, after 8 months of the intervention program implementation period. The probability of meeting the recommended levels of physical activity and fruit and vegetable intake were four- and threefold higher after the prescription of lifestyle change than only assessment and provision of advice. The procedure of engagement in and execution of the implementation strategy does not modify the effect of prescribing healthy habits (p interaction component of intervention by group, p > 0.05).</p><p><strong>Discussion: </strong>Our results show that the PVS-PREDIAPS implementation strategy manages to integrate interventions with proven efficacy in the prevention of type 2 diabetes in clinical practice in primary care. Further, they suggest that implementation outcomes were somewhat better with a sequential facilitated collaborative process focused on enhancing the autonomy and responsibility of nurses who subsequently seek a pragmatic cooperation of GPs.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov identifier: NCT03254979 . Registered 16 August 2017-retrospectively registered.</p>\",\"PeriodicalId\":417097,\"journal\":{\"name\":\"Implementation Science : IS\",\"volume\":\" \",\"pages\":\"58\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13012-021-01127-x\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation Science : IS\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13012-021-01127-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13012-021-01127-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
摘要
背景:在寻求优化实践的协作过程中,参与和指导医疗保健专业人员的最有效程序是未知的。PREDIAPS项目旨在评估不同程序的有效性和可行性,以促进跨专业协作过程,优化常规初级保健中的2型糖尿病预防。方法:在巴斯克卫生服务的9个初级保健中心进行II型混合集群随机实施试验。所有中心都接受了有效促进健康生活方式的培训。在一名当地领导和一名外部协调人的领导下,各中心实施了一个协作的结构化过程——PVS-PREDIAPS实施战略——以使干预措施及其实施适应其具体情况。这些中心被随机分配到两组中的一组:一组在全球范围内实施战略,从一开始就促进所有卫生专业人员的合作;另一组按顺序实施战略,首先以护士为中心,然后寻求医生的务实合作。以下患者符合纳入条件:所有年龄≥30岁,至少有一种已知心血管危险因素,空腹血糖水平受损(≥110-125 mg/dl),但在研究期间没有糖尿病的患者。主要结果测量涉及12个月后2型糖尿病预防实践指标的变化。结果:12个月后,3273例有2型糖尿病风险的合格患者至少看了一次家庭医生,其中490例(15%)通过评估两组患者的健康生活方式得到了解决。接受个性化生活方式改变处方的高危患者比例略高(8.6%;范围13.5-5.9% vs 6.8%;范围为7.2-5.8%),在干预计划实施8个月后,序列中心的可能性是全球中心的2.3倍(调整风险比的95% CI, 1.38-3.94)。在改变生活方式的处方之后,达到建议的身体活动水平和水果蔬菜摄入量的可能性比仅仅评估和提供建议高出四到三倍。实施策略的参与和执行过程不影响健康习惯处方的效果(p组干预交互分量,p > 0.05)。讨论:我们的研究结果表明,PVS-PREDIAPS实施策略在初级保健的临床实践中成功地整合了预防2型糖尿病的干预措施。此外,他们认为,实施结果在一定程度上更好的顺序促进协作过程侧重于加强自主权和责任的护士谁随后寻求全科医生的务实合作。试验注册:Clinicaltrials.gov标识符:NCT03254979。注册2017年8月16日-回顾性注册。
Effectiveness of two procedures for deploying a facilitated collaborative modeling implementation strategy-the PVS-PREDIAPS strategy-to optimize type 2 diabetes prevention in primary care: the PREDIAPS cluster randomized hybrid type II implementation trial.
Background: The most efficient procedures to engage and guide healthcare professionals in collaborative processes that seek to optimize practice are unknown. The PREDIAPS project aims to assess the effectiveness and feasibility of different procedures to perform a facilitated interprofessional collaborative process to optimize type 2 diabetes prevention in routine primary care.
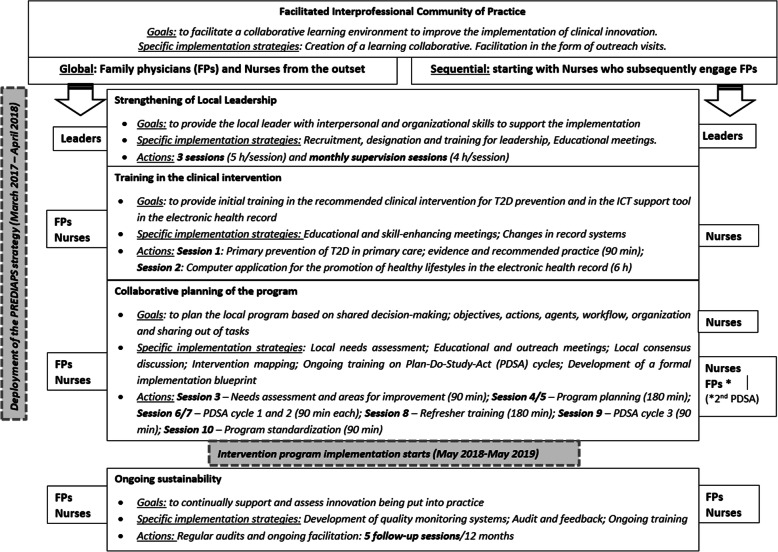
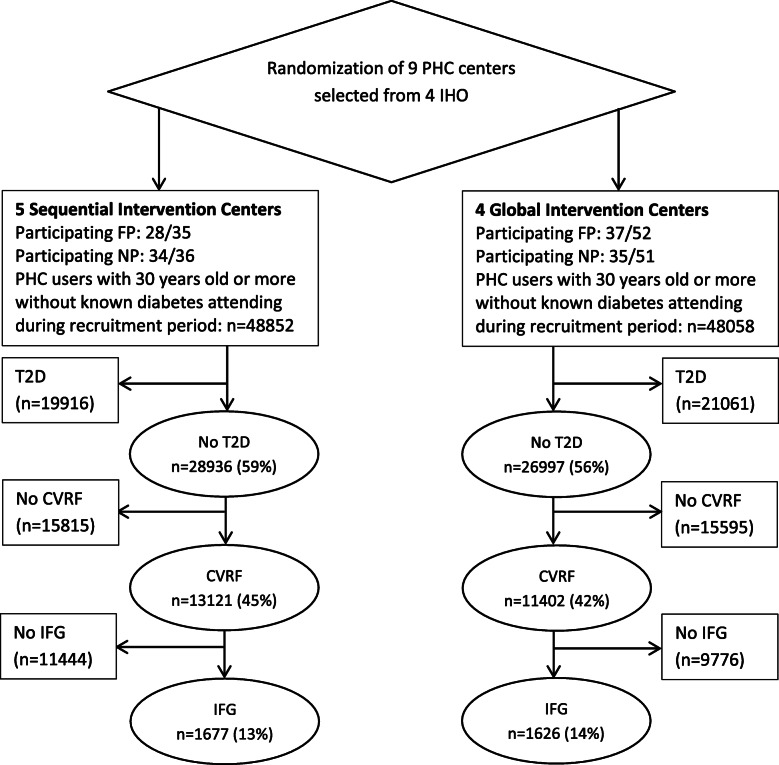
Methods: A type II hybrid cluster randomized implementation trial was conducted in nine primary care centers of the Basque Health Service. All centers received training on effective healthy lifestyle promotion. Headed by a local leader and an external facilitator, centers conducted a collaborative structured process-the PVS-PREDIAPS implementation strategy-to adapt the intervention and its implementation to their specific context. The centers were randomly allocated to one of two groups: one group applied the implementation strategy globally, promoting the cooperation of all health professionals from the beginning, and the other performed it sequentially, centered first on nurses, who later sought the pragmatic cooperation of physicians. The following patients were eligible for inclusion: all those aged ≥ 30 years old with at least one known cardiovascular risk factor and an impaired fasting glucose level (≥ 110-125 mg/dl) but without diabetes who attended centers during the study period. The main outcome measures concerned changes in type 2 diabetes prevention practice indicators after 12 months.
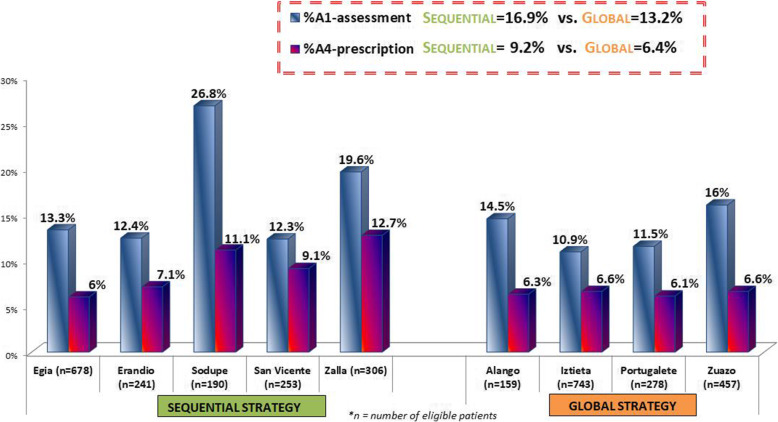
Results: After 12 months, 3273 eligible patients at risk of type 2 diabetes had attended their family physician at least once, and of these, 490 (15%) have been addressed by assessing their healthy lifestyles in both comparison groups. The proportion of at-risk patients receiving a personalized prescription of lifestyle change was slightly higher (8.6%; range 13.5-5.9% vs 6.8%; range 7.2-5.8%) and 2.3 times more likely (95% CI for adjusted hazard ratio, 1.38-3.94) in the sequential than in the global centers, after 8 months of the intervention program implementation period. The probability of meeting the recommended levels of physical activity and fruit and vegetable intake were four- and threefold higher after the prescription of lifestyle change than only assessment and provision of advice. The procedure of engagement in and execution of the implementation strategy does not modify the effect of prescribing healthy habits (p interaction component of intervention by group, p > 0.05).
Discussion: Our results show that the PVS-PREDIAPS implementation strategy manages to integrate interventions with proven efficacy in the prevention of type 2 diabetes in clinical practice in primary care. Further, they suggest that implementation outcomes were somewhat better with a sequential facilitated collaborative process focused on enhancing the autonomy and responsibility of nurses who subsequently seek a pragmatic cooperation of GPs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


