Omar A Abdel-Mannan, Celeste Manchoon, Thomas Rossor, Justine-Clair Southin, Carmen Tur, Wallace Brownlee, Susan Byrne, Manali Chitre, Alasdair Coles, Rob Forsyth, Rachel Kneen, Kshitij Mankad, Dipak Ram, Siobhan West, Sukhvir Wright, Evangeline Wassmer, Ming Lim, Olga Ciccarelli, Cheryl Hemingway, Yael Hacohen
{"title":"在英国儿童复发-缓解型多发性硬化症中使用疾病改善疗法","authors":"Omar A Abdel-Mannan, Celeste Manchoon, Thomas Rossor, Justine-Clair Southin, Carmen Tur, Wallace Brownlee, Susan Byrne, Manali Chitre, Alasdair Coles, Rob Forsyth, Rachel Kneen, Kshitij Mankad, Dipak Ram, Siobhan West, Sukhvir Wright, Evangeline Wassmer, Ming Lim, Olga Ciccarelli, Cheryl Hemingway, Yael Hacohen","doi":"10.1212/NXI.0000000000001008","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare the real-world effectiveness of newer disease-modifying therapies (DMTs) vs injectables in children with relapsing-remitting multiple sclerosis (RRMS).</p><p><strong>Methods: </strong>In this retrospective, multicenter study, from the UK Childhood Inflammatory Demyelination Network, we identified children with RRMS receiving DMTs from January 2012 to December 2018. Clinical and paraclinical data were retrieved from the medical records. Annualized relapse rates (ARRs) before and on treatment, time to relapse, time to new MRI lesions, and change in Expanded Disability Status Scale (EDSS) score were calculated.</p><p><strong>Results: </strong>Of 103 children treated with DMTs, followed up for 3.8 years, relapses on treatment were recorded in 53/89 (59.5%) on injectables vs 8/54 (15%) on newer DMTs. The ARR was reduced from 1.9 to 1.1 on injectables (<i>p</i> < 0.001) vs 1.6 to 0.3 on newer DMTs (<i>p</i> = 0.002). New MRI lesions occurred in 77/89 (86.5%) of patients on injectables vs 26/54 (47%) on newer DMTs (<i>p</i> = 0.0001). Children on newer DMTs showed longer time to relapse, time to switch treatment, and time to new radiologic activity than patients on injectables (log-rank <i>p</i> < 0.01). After adjustment for potential confounders, multivariable analysis showed that injectables were associated with 12-fold increased risk of clinical relapse (adjusted hazard ratio [HR] = 12.12, 95% CI = 1.64-89.87, <i>p</i> = 0.015) and a 2-fold increased risk of new radiologic activity (adjusted HR = 2.78, 95% CI = 1.08-7.13, <i>p</i> = 0.034) compared with newer DMTs. At 2 years from treatment initiation, 38/103 (37%) patients had MRI activity in the absence of clinical relapses. The EDSS score did not change during the follow-up, and only 2 patients had cognitive impairment.</p><p><strong>Conclusion: </strong>Newer DMTs were associated with a lower risk of clinical and radiologic relapses in patients compared with injectables. Our study adds weight to the argument for an imminent shift in practice toward the use of newer, more efficacious DMTs in the first instance.</p><p><strong>Classification of evidence: </strong>This study provides Class IV evidence that newer DMTs (oral or infusions) are superior to injectables (interferon beta/glatiramer acetate) in reducing both clinical relapses and radiologic activity in children with RRMS.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2021-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8143699/pdf/","citationCount":"0","resultStr":"{\"title\":\"Use of Disease-Modifying Therapies in Pediatric Relapsing-Remitting Multiple Sclerosis in the United Kingdom.\",\"authors\":\"Omar A Abdel-Mannan, Celeste Manchoon, Thomas Rossor, Justine-Clair Southin, Carmen Tur, Wallace Brownlee, Susan Byrne, Manali Chitre, Alasdair Coles, Rob Forsyth, Rachel Kneen, Kshitij Mankad, Dipak Ram, Siobhan West, Sukhvir Wright, Evangeline Wassmer, Ming Lim, Olga Ciccarelli, Cheryl Hemingway, Yael Hacohen\",\"doi\":\"10.1212/NXI.0000000000001008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To compare the real-world effectiveness of newer disease-modifying therapies (DMTs) vs injectables in children with relapsing-remitting multiple sclerosis (RRMS).</p><p><strong>Methods: </strong>In this retrospective, multicenter study, from the UK Childhood Inflammatory Demyelination Network, we identified children with RRMS receiving DMTs from January 2012 to December 2018. Clinical and paraclinical data were retrieved from the medical records. Annualized relapse rates (ARRs) before and on treatment, time to relapse, time to new MRI lesions, and change in Expanded Disability Status Scale (EDSS) score were calculated.</p><p><strong>Results: </strong>Of 103 children treated with DMTs, followed up for 3.8 years, relapses on treatment were recorded in 53/89 (59.5%) on injectables vs 8/54 (15%) on newer DMTs. The ARR was reduced from 1.9 to 1.1 on injectables (<i>p</i> < 0.001) vs 1.6 to 0.3 on newer DMTs (<i>p</i> = 0.002). New MRI lesions occurred in 77/89 (86.5%) of patients on injectables vs 26/54 (47%) on newer DMTs (<i>p</i> = 0.0001). Children on newer DMTs showed longer time to relapse, time to switch treatment, and time to new radiologic activity than patients on injectables (log-rank <i>p</i> < 0.01). After adjustment for potential confounders, multivariable analysis showed that injectables were associated with 12-fold increased risk of clinical relapse (adjusted hazard ratio [HR] = 12.12, 95% CI = 1.64-89.87, <i>p</i> = 0.015) and a 2-fold increased risk of new radiologic activity (adjusted HR = 2.78, 95% CI = 1.08-7.13, <i>p</i> = 0.034) compared with newer DMTs. At 2 years from treatment initiation, 38/103 (37%) patients had MRI activity in the absence of clinical relapses. The EDSS score did not change during the follow-up, and only 2 patients had cognitive impairment.</p><p><strong>Conclusion: </strong>Newer DMTs were associated with a lower risk of clinical and radiologic relapses in patients compared with injectables. Our study adds weight to the argument for an imminent shift in practice toward the use of newer, more efficacious DMTs in the first instance.</p><p><strong>Classification of evidence: </strong>This study provides Class IV evidence that newer DMTs (oral or infusions) are superior to injectables (interferon beta/glatiramer acetate) in reducing both clinical relapses and radiologic activity in children with RRMS.</p>\",\"PeriodicalId\":520720,\"journal\":{\"name\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-05-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8143699/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000001008\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/7/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000001008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/7/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:比较更新的疾病改善疗法(dmt)与注射治疗在复发-缓解型多发性硬化症(RRMS)儿童中的实际疗效。方法:在这项来自英国儿童炎症性脱髓鞘网络的回顾性多中心研究中,我们确定了2012年1月至2018年12月期间接受dmt治疗的RRMS儿童。从医疗记录中检索临床和临床旁数据。计算治疗前和治疗后的年复发率(ARRs)、复发时间、出现新MRI病变的时间以及扩展残疾状态量表(EDSS)评分的变化。结果:103名接受dmt治疗的儿童,随访3.8年,注射组有53/89例(59.5%)复发,较新的dmt组有8/54例(15%)复发。注射组的ARR从1.9降至1.1 (p < 0.001),而较新的dmt组的ARR从1.6降至0.3 (p = 0.002)。注射组患者中有77/89(86.5%)出现新的MRI病变,而较新的dmt组患者中有26/54(47%)出现新的MRI病变(p = 0.0001)。接受较新的dmt治疗的儿童比接受注射治疗的患者复发时间更长,转换治疗时间更长,接受新的放射治疗时间更长(log-rank p < 0.01)。在对潜在混杂因素进行校正后,多变量分析显示,与较新的dmt相比,注射类药物与临床复发风险增加12倍相关(校正风险比[HR] = 12.12, 95% CI = 1.64-89.87, p = 0.015),新放射活性风险增加2倍(校正风险比[HR] = 2.78, 95% CI = 1.08-7.13, p = 0.034)。在开始治疗2年后,38/103(37%)的患者在没有临床复发的情况下有MRI活动。随访期间EDSS评分无变化,仅有2例患者出现认知障碍。结论:与注射药物相比,较新的dmt与较低的临床和放射复发风险相关。我们的研究增加了在实践中立即转向使用更新,更有效的dmt的论点。证据分类:本研究提供了IV类证据,证明较新的dmt(口服或输注)在减少RRMS患儿的临床复发和放射学活性方面优于注射(干扰素/醋酸格拉替默)。
Use of Disease-Modifying Therapies in Pediatric Relapsing-Remitting Multiple Sclerosis in the United Kingdom.
Objectives: To compare the real-world effectiveness of newer disease-modifying therapies (DMTs) vs injectables in children with relapsing-remitting multiple sclerosis (RRMS).
Methods: In this retrospective, multicenter study, from the UK Childhood Inflammatory Demyelination Network, we identified children with RRMS receiving DMTs from January 2012 to December 2018. Clinical and paraclinical data were retrieved from the medical records. Annualized relapse rates (ARRs) before and on treatment, time to relapse, time to new MRI lesions, and change in Expanded Disability Status Scale (EDSS) score were calculated.
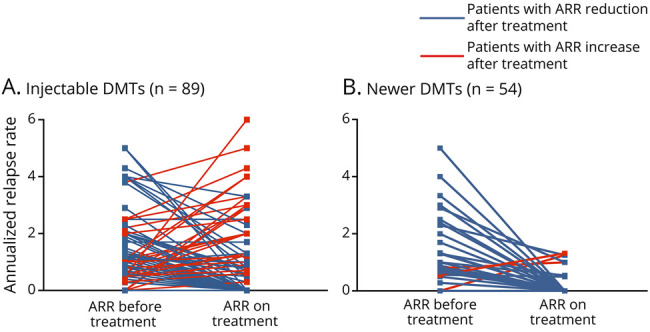
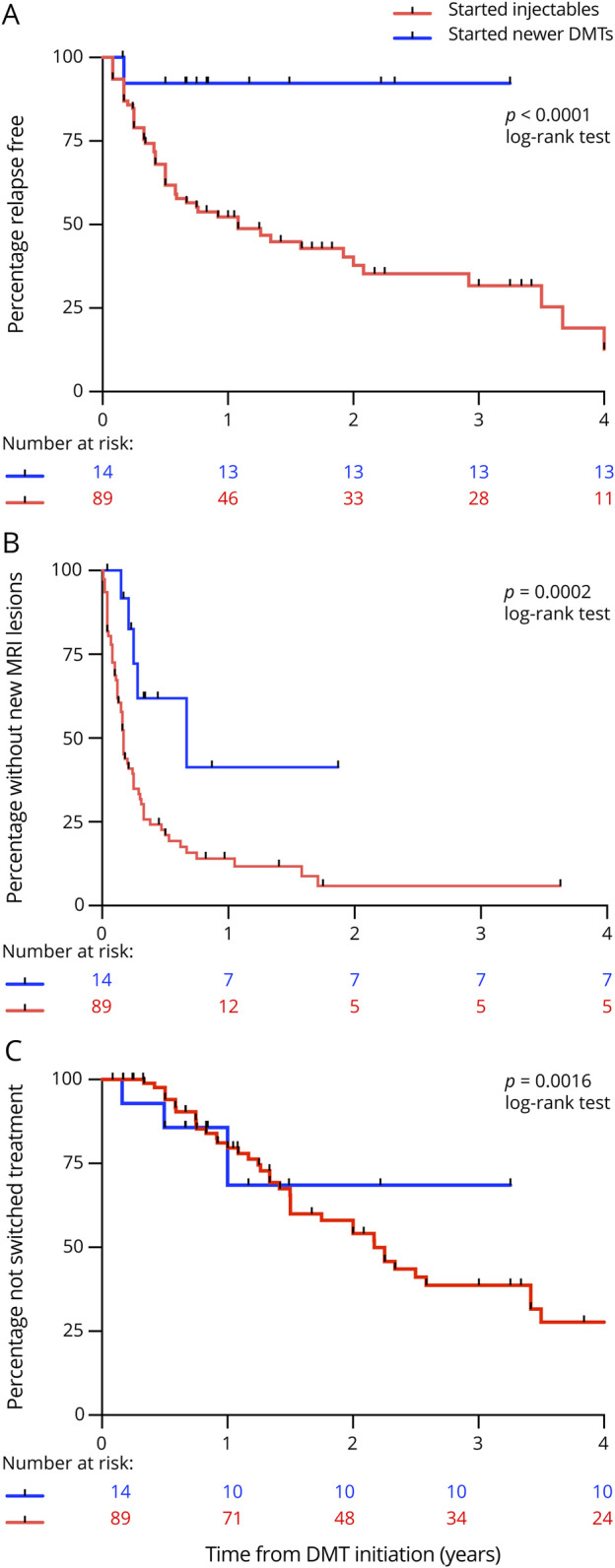
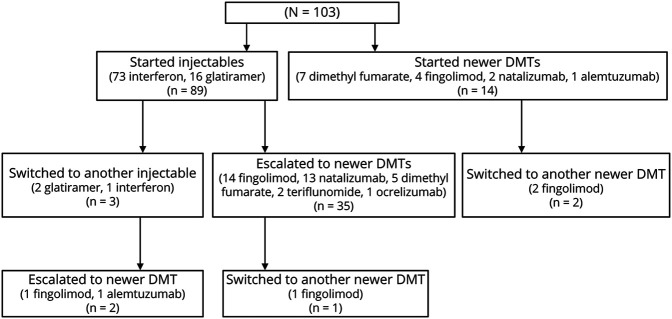
Results: Of 103 children treated with DMTs, followed up for 3.8 years, relapses on treatment were recorded in 53/89 (59.5%) on injectables vs 8/54 (15%) on newer DMTs. The ARR was reduced from 1.9 to 1.1 on injectables (p < 0.001) vs 1.6 to 0.3 on newer DMTs (p = 0.002). New MRI lesions occurred in 77/89 (86.5%) of patients on injectables vs 26/54 (47%) on newer DMTs (p = 0.0001). Children on newer DMTs showed longer time to relapse, time to switch treatment, and time to new radiologic activity than patients on injectables (log-rank p < 0.01). After adjustment for potential confounders, multivariable analysis showed that injectables were associated with 12-fold increased risk of clinical relapse (adjusted hazard ratio [HR] = 12.12, 95% CI = 1.64-89.87, p = 0.015) and a 2-fold increased risk of new radiologic activity (adjusted HR = 2.78, 95% CI = 1.08-7.13, p = 0.034) compared with newer DMTs. At 2 years from treatment initiation, 38/103 (37%) patients had MRI activity in the absence of clinical relapses. The EDSS score did not change during the follow-up, and only 2 patients had cognitive impairment.
Conclusion: Newer DMTs were associated with a lower risk of clinical and radiologic relapses in patients compared with injectables. Our study adds weight to the argument for an imminent shift in practice toward the use of newer, more efficacious DMTs in the first instance.
Classification of evidence: This study provides Class IV evidence that newer DMTs (oral or infusions) are superior to injectables (interferon beta/glatiramer acetate) in reducing both clinical relapses and radiologic activity in children with RRMS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


