Francesc Graus, Alberto Vogrig, Sergio Muñiz-Castrillo, Jean-Christophe G Antoine, Virginie Desestret, Divyanshu Dubey, Bruno Giometto, Sarosh R Irani, Bastien Joubert, Frank Leypoldt, Andrew McKeon, Harald Prüss, Dimitri Psimaras, Laure Thomas, Maarten J Titulaer, Christian A Vedeler, Jan J Verschuuren, Josep Dalmau, Jerome Honnorat
{"title":"副肿瘤神经综合征的最新诊断标准。","authors":"Francesc Graus, Alberto Vogrig, Sergio Muñiz-Castrillo, Jean-Christophe G Antoine, Virginie Desestret, Divyanshu Dubey, Bruno Giometto, Sarosh R Irani, Bastien Joubert, Frank Leypoldt, Andrew McKeon, Harald Prüss, Dimitri Psimaras, Laure Thomas, Maarten J Titulaer, Christian A Vedeler, Jan J Verschuuren, Josep Dalmau, Jerome Honnorat","doi":"10.1212/NXI.0000000000001014","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The contemporary diagnosis of paraneoplastic neurologic syndromes (PNSs) requires an increasing understanding of their clinical, immunologic, and oncologic heterogeneity. The 2004 PNS criteria are partially outdated due to advances in PNS research in the last 16 years leading to the identification of new phenotypes and antibodies that have transformed the diagnostic approach to PNS. Here, we propose updated diagnostic criteria for PNS.</p><p><strong>Methods: </strong>A panel of experts developed by consensus a modified set of diagnostic PNS criteria for clinical decision making and research purposes. The panel reappraised the 2004 criteria alongside new knowledge on PNS obtained from published and unpublished data generated by the different laboratories involved in the project.</p><p><strong>Results: </strong>The panel proposed to substitute \"classical syndromes\" with the term \"high-risk phenotypes\" for cancer and introduce the concept of \"intermediate-risk phenotypes.\" The term \"onconeural antibody\" was replaced by \"high risk\" (>70% associated with cancer) and \"intermediate risk\" (30%-70% associated with cancer) antibodies. The panel classified 3 levels of evidence for PNS: definite, probable, and possible. Each level can be reached by using the PNS-Care Score, which combines clinical phenotype, antibody type, the presence or absence of cancer, and time of follow-up. With the exception of opsoclonus-myoclonus, the diagnosis of definite PNS requires the presence of high- or intermediate-risk antibodies. Specific recommendations for similar syndromes triggered by immune checkpoint inhibitors are also provided.</p><p><strong>Conclusions: </strong>The proposed criteria and recommendations should be used to enhance the clinical care of patients with PNS and to encourage standardization of research initiatives addressing PNS.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2021-05-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8237398/pdf/","citationCount":"0","resultStr":"{\"title\":\"Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes.\",\"authors\":\"Francesc Graus, Alberto Vogrig, Sergio Muñiz-Castrillo, Jean-Christophe G Antoine, Virginie Desestret, Divyanshu Dubey, Bruno Giometto, Sarosh R Irani, Bastien Joubert, Frank Leypoldt, Andrew McKeon, Harald Prüss, Dimitri Psimaras, Laure Thomas, Maarten J Titulaer, Christian A Vedeler, Jan J Verschuuren, Josep Dalmau, Jerome Honnorat\",\"doi\":\"10.1212/NXI.0000000000001014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The contemporary diagnosis of paraneoplastic neurologic syndromes (PNSs) requires an increasing understanding of their clinical, immunologic, and oncologic heterogeneity. The 2004 PNS criteria are partially outdated due to advances in PNS research in the last 16 years leading to the identification of new phenotypes and antibodies that have transformed the diagnostic approach to PNS. Here, we propose updated diagnostic criteria for PNS.</p><p><strong>Methods: </strong>A panel of experts developed by consensus a modified set of diagnostic PNS criteria for clinical decision making and research purposes. The panel reappraised the 2004 criteria alongside new knowledge on PNS obtained from published and unpublished data generated by the different laboratories involved in the project.</p><p><strong>Results: </strong>The panel proposed to substitute \\\"classical syndromes\\\" with the term \\\"high-risk phenotypes\\\" for cancer and introduce the concept of \\\"intermediate-risk phenotypes.\\\" The term \\\"onconeural antibody\\\" was replaced by \\\"high risk\\\" (>70% associated with cancer) and \\\"intermediate risk\\\" (30%-70% associated with cancer) antibodies. The panel classified 3 levels of evidence for PNS: definite, probable, and possible. Each level can be reached by using the PNS-Care Score, which combines clinical phenotype, antibody type, the presence or absence of cancer, and time of follow-up. With the exception of opsoclonus-myoclonus, the diagnosis of definite PNS requires the presence of high- or intermediate-risk antibodies. Specific recommendations for similar syndromes triggered by immune checkpoint inhibitors are also provided.</p><p><strong>Conclusions: </strong>The proposed criteria and recommendations should be used to enhance the clinical care of patients with PNS and to encourage standardization of research initiatives addressing PNS.</p>\",\"PeriodicalId\":520720,\"journal\":{\"name\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-05-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8237398/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000001014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/7/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000001014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/7/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes.
Objective: The contemporary diagnosis of paraneoplastic neurologic syndromes (PNSs) requires an increasing understanding of their clinical, immunologic, and oncologic heterogeneity. The 2004 PNS criteria are partially outdated due to advances in PNS research in the last 16 years leading to the identification of new phenotypes and antibodies that have transformed the diagnostic approach to PNS. Here, we propose updated diagnostic criteria for PNS.
Methods: A panel of experts developed by consensus a modified set of diagnostic PNS criteria for clinical decision making and research purposes. The panel reappraised the 2004 criteria alongside new knowledge on PNS obtained from published and unpublished data generated by the different laboratories involved in the project.
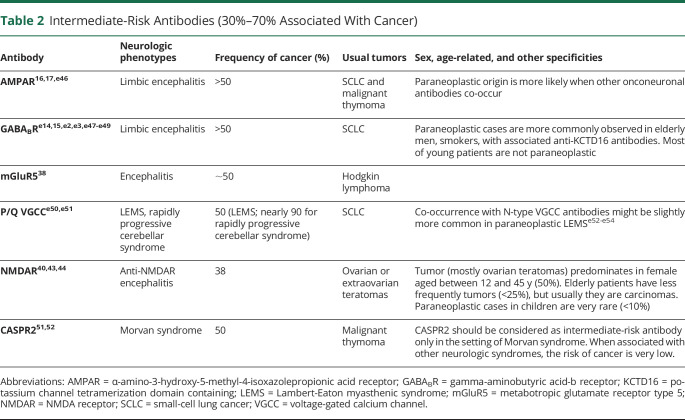
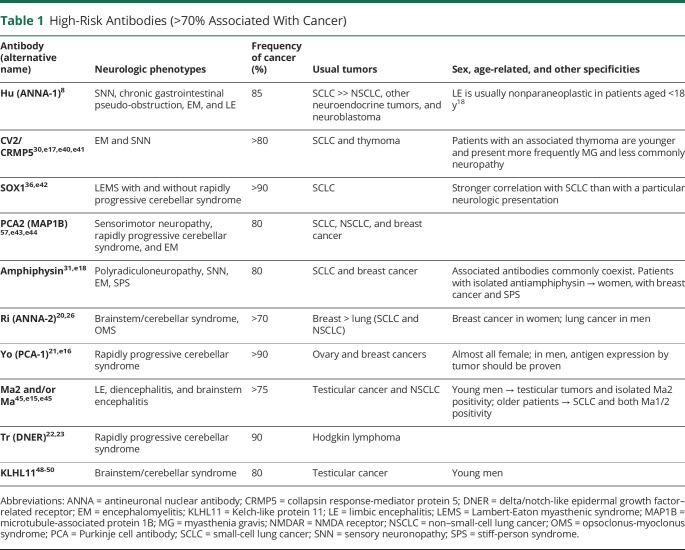
Results: The panel proposed to substitute "classical syndromes" with the term "high-risk phenotypes" for cancer and introduce the concept of "intermediate-risk phenotypes." The term "onconeural antibody" was replaced by "high risk" (>70% associated with cancer) and "intermediate risk" (30%-70% associated with cancer) antibodies. The panel classified 3 levels of evidence for PNS: definite, probable, and possible. Each level can be reached by using the PNS-Care Score, which combines clinical phenotype, antibody type, the presence or absence of cancer, and time of follow-up. With the exception of opsoclonus-myoclonus, the diagnosis of definite PNS requires the presence of high- or intermediate-risk antibodies. Specific recommendations for similar syndromes triggered by immune checkpoint inhibitors are also provided.
Conclusions: The proposed criteria and recommendations should be used to enhance the clinical care of patients with PNS and to encourage standardization of research initiatives addressing PNS.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


