Myrlene Sanon Aigbogun, Robert A Stellhorn, Christina S Pao, Stephen L Seliger
{"title":"常染色体显性多囊肾病的x线影像分析。","authors":"Myrlene Sanon Aigbogun, Robert A Stellhorn, Christina S Pao, Stephen L Seliger","doi":"10.2147/IJNRD.S300331","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Progression of autosomal dominant polycystic kidney disease (ADPKD) is highly variable, with some patients progressing rapidly to end-stage renal disease (ESRD). Abdominal imaging is an important modality for verifying diagnosis in patients at risk for rapidly progressing ADPKD, targeting them for early treatment that could slow onset of ESRD. Published literature is limited on the real-world abdominal imaging utilization patterns in ADPKD.</p><p><strong>Methods: </strong>A retrospective healthcare administrative claims analysis examining abdominal imaging scans occurring from January 1, 2014, through June 30, 2017, was conducted using the IBM MarketScan<sup>®</sup> commercial and Medicare supplemental databases. Patients in the United States who were at least 18 years old and had at least 1 inpatient claim or 2 outpatient claims (with different dates of service) with an ADPKD diagnosis code, as defined by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM codes 753.12 [polycystic kidney, unspecified type] and 753.13 [polycystic kidney, autosomal dominant] and/or Tenth Revision (ICD-10-CM codes Q61.2 [polycystic kidney, adult type] and Q61.3 [polycystic kidney, unspecified]) were included.</p><p><strong>Results: </strong>Of the 4637 patients with ADPKD (mean age, 51.2 years [SD = 15.52]), 59% had ≥1 abdominal imaging scan. Of these patients, 46% had ≥1 computed tomography (CT) scan, 25% had ≥1 ultrasound, 10% had ≥1 magnetic resonance imaging scan. Among the 1754 patients (38%) with chronic kidney disease (CKD) stage information, CT imaging was more frequent in later stages (31% stage 1 versus 68% stage 5). The proportion of patients undergoing at least 1 CT or MRI scan increased with disease severity (37% in stage 1, 42% in stage 2, 48% in stage 3, 56% in stage 4, and 71% in stage 5).</p><p><strong>Conclusion: </strong>Results of this analysis support the need for further investigation into abdominal imaging utilization in managing patients with ADPKD. Future research could clarify barriers and increase access to imaging, which has the potential to inform risk stratification, help patients delay dialysis or transplantation associated with ESRD, and help health systems avoid the costs associated with ESRD.</p>","PeriodicalId":14181,"journal":{"name":"International Journal of Nephrology and Renovascular Disease","volume":"14 ","pages":"133-142"},"PeriodicalIF":2.1000,"publicationDate":"2021-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fe/64/ijnrd-14-133.PMC8112873.pdf","citationCount":"0","resultStr":"{\"title\":\"Radiographic Imaging in Autosomal Dominant Polycystic Kidney Disease: A Claims Analysis.\",\"authors\":\"Myrlene Sanon Aigbogun, Robert A Stellhorn, Christina S Pao, Stephen L Seliger\",\"doi\":\"10.2147/IJNRD.S300331\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Progression of autosomal dominant polycystic kidney disease (ADPKD) is highly variable, with some patients progressing rapidly to end-stage renal disease (ESRD). Abdominal imaging is an important modality for verifying diagnosis in patients at risk for rapidly progressing ADPKD, targeting them for early treatment that could slow onset of ESRD. Published literature is limited on the real-world abdominal imaging utilization patterns in ADPKD.</p><p><strong>Methods: </strong>A retrospective healthcare administrative claims analysis examining abdominal imaging scans occurring from January 1, 2014, through June 30, 2017, was conducted using the IBM MarketScan<sup>®</sup> commercial and Medicare supplemental databases. Patients in the United States who were at least 18 years old and had at least 1 inpatient claim or 2 outpatient claims (with different dates of service) with an ADPKD diagnosis code, as defined by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM codes 753.12 [polycystic kidney, unspecified type] and 753.13 [polycystic kidney, autosomal dominant] and/or Tenth Revision (ICD-10-CM codes Q61.2 [polycystic kidney, adult type] and Q61.3 [polycystic kidney, unspecified]) were included.</p><p><strong>Results: </strong>Of the 4637 patients with ADPKD (mean age, 51.2 years [SD = 15.52]), 59% had ≥1 abdominal imaging scan. Of these patients, 46% had ≥1 computed tomography (CT) scan, 25% had ≥1 ultrasound, 10% had ≥1 magnetic resonance imaging scan. Among the 1754 patients (38%) with chronic kidney disease (CKD) stage information, CT imaging was more frequent in later stages (31% stage 1 versus 68% stage 5). The proportion of patients undergoing at least 1 CT or MRI scan increased with disease severity (37% in stage 1, 42% in stage 2, 48% in stage 3, 56% in stage 4, and 71% in stage 5).</p><p><strong>Conclusion: </strong>Results of this analysis support the need for further investigation into abdominal imaging utilization in managing patients with ADPKD. Future research could clarify barriers and increase access to imaging, which has the potential to inform risk stratification, help patients delay dialysis or transplantation associated with ESRD, and help health systems avoid the costs associated with ESRD.</p>\",\"PeriodicalId\":14181,\"journal\":{\"name\":\"International Journal of Nephrology and Renovascular Disease\",\"volume\":\"14 \",\"pages\":\"133-142\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2021-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fe/64/ijnrd-14-133.PMC8112873.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Nephrology and Renovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/IJNRD.S300331\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Nephrology and Renovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IJNRD.S300331","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Radiographic Imaging in Autosomal Dominant Polycystic Kidney Disease: A Claims Analysis.
Background: Progression of autosomal dominant polycystic kidney disease (ADPKD) is highly variable, with some patients progressing rapidly to end-stage renal disease (ESRD). Abdominal imaging is an important modality for verifying diagnosis in patients at risk for rapidly progressing ADPKD, targeting them for early treatment that could slow onset of ESRD. Published literature is limited on the real-world abdominal imaging utilization patterns in ADPKD.
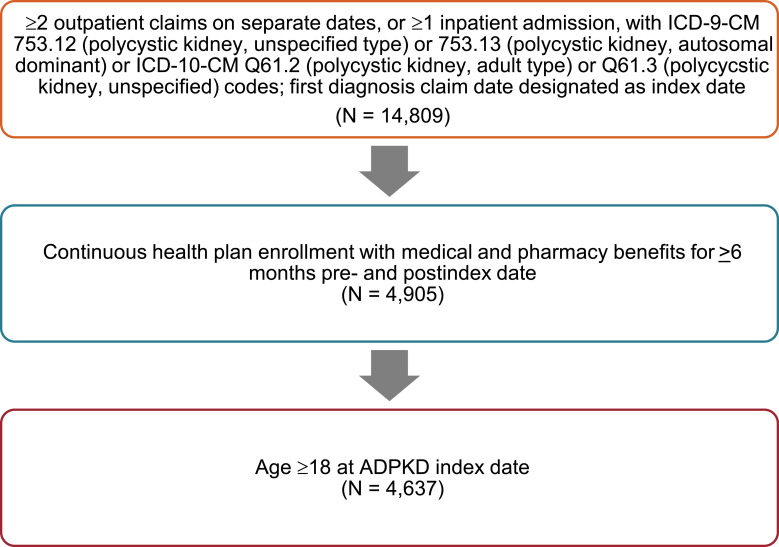
Methods: A retrospective healthcare administrative claims analysis examining abdominal imaging scans occurring from January 1, 2014, through June 30, 2017, was conducted using the IBM MarketScan® commercial and Medicare supplemental databases. Patients in the United States who were at least 18 years old and had at least 1 inpatient claim or 2 outpatient claims (with different dates of service) with an ADPKD diagnosis code, as defined by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM codes 753.12 [polycystic kidney, unspecified type] and 753.13 [polycystic kidney, autosomal dominant] and/or Tenth Revision (ICD-10-CM codes Q61.2 [polycystic kidney, adult type] and Q61.3 [polycystic kidney, unspecified]) were included.
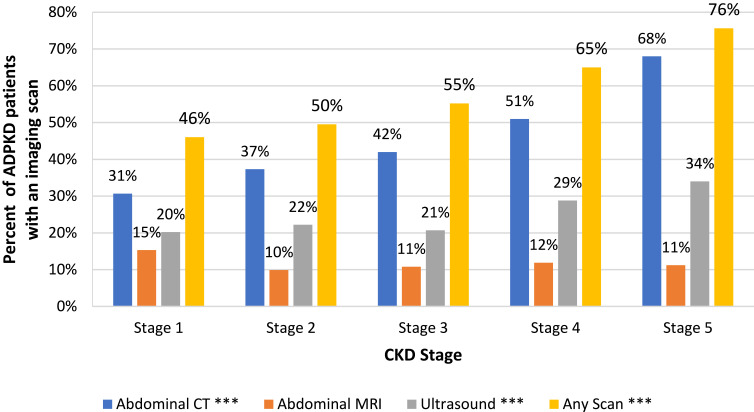
Results: Of the 4637 patients with ADPKD (mean age, 51.2 years [SD = 15.52]), 59% had ≥1 abdominal imaging scan. Of these patients, 46% had ≥1 computed tomography (CT) scan, 25% had ≥1 ultrasound, 10% had ≥1 magnetic resonance imaging scan. Among the 1754 patients (38%) with chronic kidney disease (CKD) stage information, CT imaging was more frequent in later stages (31% stage 1 versus 68% stage 5). The proportion of patients undergoing at least 1 CT or MRI scan increased with disease severity (37% in stage 1, 42% in stage 2, 48% in stage 3, 56% in stage 4, and 71% in stage 5).
Conclusion: Results of this analysis support the need for further investigation into abdominal imaging utilization in managing patients with ADPKD. Future research could clarify barriers and increase access to imaging, which has the potential to inform risk stratification, help patients delay dialysis or transplantation associated with ESRD, and help health systems avoid the costs associated with ESRD.
期刊介绍:
International Journal of Nephrology and Renovascular Disease is an international, peer-reviewed, open-access journal focusing on the pathophysiology of the kidney and vascular supply. Epidemiology, screening, diagnosis, and treatment interventions are covered as well as basic science, biochemical and immunological studies. In particular, emphasis will be given to: -Chronic kidney disease- Complications of renovascular disease- Imaging techniques- Renal hypertension- Renal cancer- Treatment including pharmacological and transplantation- Dialysis and treatment of complications of dialysis and renal disease- Quality of Life- Patient satisfaction and preference- Health economic evaluations. The journal welcomes submitted papers covering original research, basic science, clinical studies, reviews & evaluations, guidelines, expert opinion and commentary, case reports and extended reports. The main focus of the journal will be to publish research and clinical results in humans but preclinical, animal and in vitro studies will be published where they shed light on disease processes and potential new therapies and interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


