Suhyun Shim, Kyung Min Park, Youn Jee Chung, Mee Ran Kim
{"title":"绝经期泌尿生殖系统综合征的最新治疗选择:激素和非激素管理。","authors":"Suhyun Shim, Kyung Min Park, Youn Jee Chung, Mee Ran Kim","doi":"10.6118/jmm.20034","DOIUrl":null,"url":null,"abstract":"<p><p>Postmenopausal atrophic vaginitis, along with vasomotor symptoms and sleep disorders, is one of the most troublesome symptoms of menopause. However, many women do not manage this symptom properly due to insufficient knowledge of the symptoms or sexual embarrassment. With appropriate treatment, many postmenopausal women can experience relief from discomforts, including burning sensation or dryness of the vagina and dyspareunia. Topical lubricants and moisturizers, systemic and local estrogens, testosterones, intravaginal dehydroepiandrosterones (DHEAs), selective estrogen receptor modulators, and energy-based therapies are possible treatment modalities. Systemic and local estrogen therapies effectively treat genitourinary syndrome of menopause (GSM), but they are contraindicated in patients with breast cancer, for whom lubricants and moisturizers must be considered as the primary treatment. Intravaginal DHEA and ospemifene can be recommended for moderate to severe GSM; however, there is insufficient data on the use of intravaginal DHEA or ospemifene in patients with breast cancer, and further studies are needed. Energy-based devices such as vaginal laser therapy reportedly alleviate GSM symptoms; however, the U.S. Food and Drug Administration warning has recently been issued because of complications such as chronic pain and burning sensations of the vagina. To summarize, clinicians should provide appropriate individualized treatment options depending on women's past history, symptom severity, and chief complaints.</p>","PeriodicalId":16410,"journal":{"name":"Journal of Menopausal Medicine","volume":"27 1","pages":"1-7"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/8f/jmm-27-1.PMC8102810.pdf","citationCount":"10","resultStr":"{\"title\":\"Updates on Therapeutic Alternatives for Genitourinary Syndrome of Menopause: Hormonal and Non-Hormonal Managements.\",\"authors\":\"Suhyun Shim, Kyung Min Park, Youn Jee Chung, Mee Ran Kim\",\"doi\":\"10.6118/jmm.20034\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Postmenopausal atrophic vaginitis, along with vasomotor symptoms and sleep disorders, is one of the most troublesome symptoms of menopause. However, many women do not manage this symptom properly due to insufficient knowledge of the symptoms or sexual embarrassment. With appropriate treatment, many postmenopausal women can experience relief from discomforts, including burning sensation or dryness of the vagina and dyspareunia. Topical lubricants and moisturizers, systemic and local estrogens, testosterones, intravaginal dehydroepiandrosterones (DHEAs), selective estrogen receptor modulators, and energy-based therapies are possible treatment modalities. Systemic and local estrogen therapies effectively treat genitourinary syndrome of menopause (GSM), but they are contraindicated in patients with breast cancer, for whom lubricants and moisturizers must be considered as the primary treatment. Intravaginal DHEA and ospemifene can be recommended for moderate to severe GSM; however, there is insufficient data on the use of intravaginal DHEA or ospemifene in patients with breast cancer, and further studies are needed. Energy-based devices such as vaginal laser therapy reportedly alleviate GSM symptoms; however, the U.S. Food and Drug Administration warning has recently been issued because of complications such as chronic pain and burning sensations of the vagina. To summarize, clinicians should provide appropriate individualized treatment options depending on women's past history, symptom severity, and chief complaints.</p>\",\"PeriodicalId\":16410,\"journal\":{\"name\":\"Journal of Menopausal Medicine\",\"volume\":\"27 1\",\"pages\":\"1-7\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/8f/jmm-27-1.PMC8102810.pdf\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Menopausal Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.6118/jmm.20034\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Menopausal Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.6118/jmm.20034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Updates on Therapeutic Alternatives for Genitourinary Syndrome of Menopause: Hormonal and Non-Hormonal Managements.
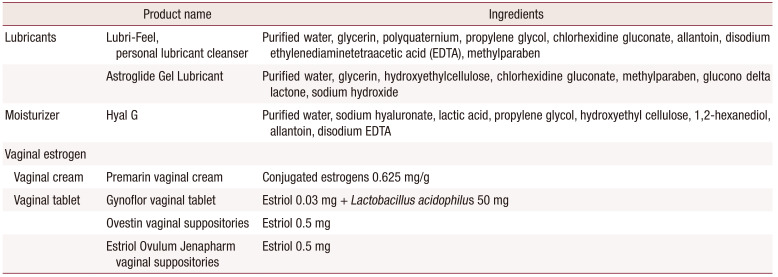
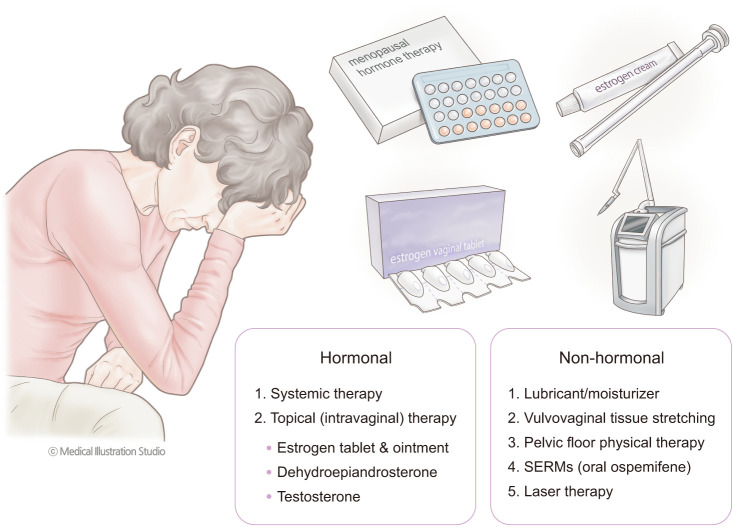
Postmenopausal atrophic vaginitis, along with vasomotor symptoms and sleep disorders, is one of the most troublesome symptoms of menopause. However, many women do not manage this symptom properly due to insufficient knowledge of the symptoms or sexual embarrassment. With appropriate treatment, many postmenopausal women can experience relief from discomforts, including burning sensation or dryness of the vagina and dyspareunia. Topical lubricants and moisturizers, systemic and local estrogens, testosterones, intravaginal dehydroepiandrosterones (DHEAs), selective estrogen receptor modulators, and energy-based therapies are possible treatment modalities. Systemic and local estrogen therapies effectively treat genitourinary syndrome of menopause (GSM), but they are contraindicated in patients with breast cancer, for whom lubricants and moisturizers must be considered as the primary treatment. Intravaginal DHEA and ospemifene can be recommended for moderate to severe GSM; however, there is insufficient data on the use of intravaginal DHEA or ospemifene in patients with breast cancer, and further studies are needed. Energy-based devices such as vaginal laser therapy reportedly alleviate GSM symptoms; however, the U.S. Food and Drug Administration warning has recently been issued because of complications such as chronic pain and burning sensations of the vagina. To summarize, clinicians should provide appropriate individualized treatment options depending on women's past history, symptom severity, and chief complaints.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


