Jan Van Elslande, Samira Hijjit, Katrien De Vusser, Michel Langlois, Björn Meijers, Ann Mertens, Bart Van der Schueren, Glynis Frans, Pieter Vermeersch
{"title":"延迟诊断和治疗极端高甘油三酯血症由于排斥血脂样本。","authors":"Jan Van Elslande, Samira Hijjit, Katrien De Vusser, Michel Langlois, Björn Meijers, Ann Mertens, Bart Van der Schueren, Glynis Frans, Pieter Vermeersch","doi":"10.11613/BM.2021.021002","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Most laboratories routinely determine haemolysis, icterus and lipemia indices to identify lipemic samples and reject potentially affected results. Hypertriglyceridemia is the most common cause of lipemia and severe hypertriglyceridemia (≥ 11.3 mmol/L) is a major risk factor of acute pancreatitis.</p><p><strong>Laboratory analysis: </strong>A 56-year-old woman attended the outpatient clinic for a follow-up visit 1 month after a kidney transplantation. Her immunosuppressive therapy consisted of corticosteroids, cyclosporine, and mycophenolic acid. The routine clinical chemistry sample was rejected due to extreme lipemia. The comment \"extreme lipemic sample\" was added on the report, but the requesting physician could not be reached. The Cobas 8000 gave a technical error (absorption > 3.3) for the HIL-indices (L-index: 38.6 mmol/L) which persisted after high-speed centrifugation. The patient was given a new appointment 2 days later. The new sample was also grossly lipemic and gave the same technical error (L-index: 35.9 mmol/L).</p><p><strong>What happened: </strong>The second sample was manually diluted 20-fold after centrifugation to obtain a result for triglycerides within the measuring range (0.10-50.0 mmol/L). Triglycerides were 169.1 mmol/L, corresponding to very severe hypertriglyceridemia. This result was communicated to the nephrologist and the patient immediately recalled to the hospital. She received therapeutic plasma exchange the next day and did not develop acute pancreatitis.</p><p><strong>Main lesson: </strong>This case illustrates the delicate balance between avoiding the release of unreliable results due to lipemia and the risk of delayed diagnosis when results are rejected. Providing an estimate of the degree of hypertriglyceridemia might be preferable to rejecting the result.</p>","PeriodicalId":9021,"journal":{"name":"Biochemia Medica","volume":"31 2","pages":"021002"},"PeriodicalIF":3.8000,"publicationDate":"2021-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8047784/pdf/","citationCount":"1","resultStr":"{\"title\":\"Delayed diagnosis and treatment of extreme hypertriglyceridemia due to rejection of a lipemic sample.\",\"authors\":\"Jan Van Elslande, Samira Hijjit, Katrien De Vusser, Michel Langlois, Björn Meijers, Ann Mertens, Bart Van der Schueren, Glynis Frans, Pieter Vermeersch\",\"doi\":\"10.11613/BM.2021.021002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Most laboratories routinely determine haemolysis, icterus and lipemia indices to identify lipemic samples and reject potentially affected results. Hypertriglyceridemia is the most common cause of lipemia and severe hypertriglyceridemia (≥ 11.3 mmol/L) is a major risk factor of acute pancreatitis.</p><p><strong>Laboratory analysis: </strong>A 56-year-old woman attended the outpatient clinic for a follow-up visit 1 month after a kidney transplantation. Her immunosuppressive therapy consisted of corticosteroids, cyclosporine, and mycophenolic acid. The routine clinical chemistry sample was rejected due to extreme lipemia. The comment \\\"extreme lipemic sample\\\" was added on the report, but the requesting physician could not be reached. The Cobas 8000 gave a technical error (absorption > 3.3) for the HIL-indices (L-index: 38.6 mmol/L) which persisted after high-speed centrifugation. The patient was given a new appointment 2 days later. The new sample was also grossly lipemic and gave the same technical error (L-index: 35.9 mmol/L).</p><p><strong>What happened: </strong>The second sample was manually diluted 20-fold after centrifugation to obtain a result for triglycerides within the measuring range (0.10-50.0 mmol/L). Triglycerides were 169.1 mmol/L, corresponding to very severe hypertriglyceridemia. This result was communicated to the nephrologist and the patient immediately recalled to the hospital. She received therapeutic plasma exchange the next day and did not develop acute pancreatitis.</p><p><strong>Main lesson: </strong>This case illustrates the delicate balance between avoiding the release of unreliable results due to lipemia and the risk of delayed diagnosis when results are rejected. Providing an estimate of the degree of hypertriglyceridemia might be preferable to rejecting the result.</p>\",\"PeriodicalId\":9021,\"journal\":{\"name\":\"Biochemia Medica\",\"volume\":\"31 2\",\"pages\":\"021002\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2021-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8047784/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biochemia Medica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.11613/BM.2021.021002\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/4/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICAL LABORATORY TECHNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biochemia Medica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.11613/BM.2021.021002","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/4/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICAL LABORATORY TECHNOLOGY","Score":null,"Total":0}
Delayed diagnosis and treatment of extreme hypertriglyceridemia due to rejection of a lipemic sample.
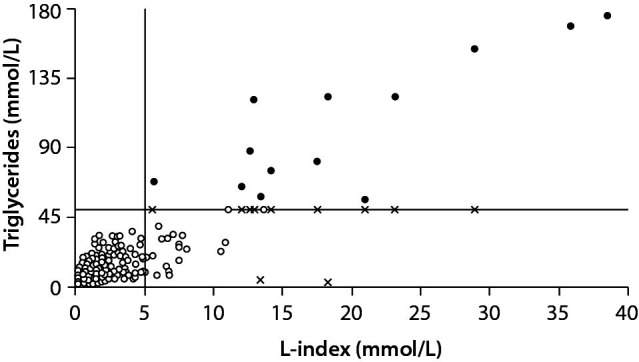
Introduction: Most laboratories routinely determine haemolysis, icterus and lipemia indices to identify lipemic samples and reject potentially affected results. Hypertriglyceridemia is the most common cause of lipemia and severe hypertriglyceridemia (≥ 11.3 mmol/L) is a major risk factor of acute pancreatitis.
Laboratory analysis: A 56-year-old woman attended the outpatient clinic for a follow-up visit 1 month after a kidney transplantation. Her immunosuppressive therapy consisted of corticosteroids, cyclosporine, and mycophenolic acid. The routine clinical chemistry sample was rejected due to extreme lipemia. The comment "extreme lipemic sample" was added on the report, but the requesting physician could not be reached. The Cobas 8000 gave a technical error (absorption > 3.3) for the HIL-indices (L-index: 38.6 mmol/L) which persisted after high-speed centrifugation. The patient was given a new appointment 2 days later. The new sample was also grossly lipemic and gave the same technical error (L-index: 35.9 mmol/L).
What happened: The second sample was manually diluted 20-fold after centrifugation to obtain a result for triglycerides within the measuring range (0.10-50.0 mmol/L). Triglycerides were 169.1 mmol/L, corresponding to very severe hypertriglyceridemia. This result was communicated to the nephrologist and the patient immediately recalled to the hospital. She received therapeutic plasma exchange the next day and did not develop acute pancreatitis.
Main lesson: This case illustrates the delicate balance between avoiding the release of unreliable results due to lipemia and the risk of delayed diagnosis when results are rejected. Providing an estimate of the degree of hypertriglyceridemia might be preferable to rejecting the result.
期刊介绍:
Biochemia Medica is the official peer-reviewed journal of the Croatian Society of Medical Biochemistry and Laboratory Medicine. Journal provides a wide coverage of research in all aspects of clinical chemistry and laboratory medicine. Following categories fit into the scope of the Journal: general clinical chemistry, haematology and haemostasis, molecular diagnostics and endocrinology. Development, validation and verification of analytical techniques and methods applicable to clinical chemistry and laboratory medicine are welcome as well as studies dealing with laboratory organization, automation and quality control. Journal publishes on a regular basis educative preanalytical case reports (Preanalytical mysteries), articles dealing with applied biostatistics (Lessons in biostatistics) and research integrity (Research integrity corner).


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


