Jessica Hier, Galit Avior, Marc Pusztaszeri, Joshua R Krasner, Noura Alyouha, Veronique-Isabelle Forest, Michael P Hier, Alex Mlynarek, Keith Richardson, Nader Sadeghi, Michael Tamilia, Richard J Payne
{"title":"分子检测细胞学可疑和恶性(Bethesda V和VI)甲状腺结节优化手术干预的程度:回顾性图表回顾。","authors":"Jessica Hier, Galit Avior, Marc Pusztaszeri, Joshua R Krasner, Noura Alyouha, Veronique-Isabelle Forest, Michael P Hier, Alex Mlynarek, Keith Richardson, Nader Sadeghi, Michael Tamilia, Richard J Payne","doi":"10.1186/s40463-021-00500-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Molecular testing has been used for cytologically indeterminate thyroid nodules (Bethesda III and IV), where the risk of malignancy is 10-40%. However, to date, the role of molecular testing in cytologically suspicious or positive for malignancy (Bethesda V and VI) thyroid nodules has been controversial. The aim of this study was to determine whether patients who had molecular testing in Bethesda V and VI thyroid nodules had the optimal extent of surgery performed more often than patients who did not have molecular testing performed.</p><p><strong>Methods: </strong>A retrospective chart review of 122 cases was performed: 101 patients from the McGill University teaching hospitals and 21 patients from the Hillel Yaffe Medical center, Technion University. Patients included in the study were those with Bethesda V or VI thyroid nodules who underwent molecular testing (ThyGenext® or ThyroseqV3®) (McGill n = 72, Hillel Yaffe n = 14). Patients with Bethesda V or VI thyroid nodules who did not undergo molecular testing were used as controls (McGill n = 29, Hillel Yaffe n = 7). Each case was reviewed in order to determine whether the patient had optimal surgery. This was defined as total thyroidectomy in the presence of either a positive lymph node, extrathyroidal extension, or an aggressive pathological variant of papillary thyroid carcinoma (tall cell, hobnail, columnar cell, diffuse sclerosing, and solid/trabecular) documented on the final pathology report. In all other cases, a lobectomy/hemi/subtotal thyroidectomy was considered as optimal surgery. Chi-squared testing was performed to compare groups.</p><p><strong>Results: </strong>When molecular testing was done, 91.86% (79/86) of surgeries in the molecular testing group were optimal, compared to 61.11% (22/36) in the control group. At McGill University teaching hospitals and at Hillel Yaffe, 91.67% (66/72) and 92.86% (13/14) of surgeries in the intervention group were considered as optimal, respectively. This compares to 58.62% (17/29) at McGill and 71.43% (5/7) at Hillel Yaffe when molecular testing was not performed (p = .001, p = .186).</p><p><strong>Conclusions: </strong>In this study, molecular testing in Bethesda V and VI thyroid tumors significantly improved the likelihood of optimal surgery. Therefore, molecular testing may have an important role in optimizing surgical procedures performed in the setting of Bethesda V and VI thyroid nodules. Prospective studies with larger sample sizes are required to further investigate this finding.</p>","PeriodicalId":520683,"journal":{"name":"Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale","volume":" ","pages":"29"},"PeriodicalIF":2.2000,"publicationDate":"2021-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40463-021-00500-6","citationCount":"8","resultStr":"{\"title\":\"Molecular testing for cytologically suspicious and malignant (Bethesda V and VI) thyroid nodules to optimize the extent of surgical intervention: a retrospective chart review.\",\"authors\":\"Jessica Hier, Galit Avior, Marc Pusztaszeri, Joshua R Krasner, Noura Alyouha, Veronique-Isabelle Forest, Michael P Hier, Alex Mlynarek, Keith Richardson, Nader Sadeghi, Michael Tamilia, Richard J Payne\",\"doi\":\"10.1186/s40463-021-00500-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Molecular testing has been used for cytologically indeterminate thyroid nodules (Bethesda III and IV), where the risk of malignancy is 10-40%. However, to date, the role of molecular testing in cytologically suspicious or positive for malignancy (Bethesda V and VI) thyroid nodules has been controversial. The aim of this study was to determine whether patients who had molecular testing in Bethesda V and VI thyroid nodules had the optimal extent of surgery performed more often than patients who did not have molecular testing performed.</p><p><strong>Methods: </strong>A retrospective chart review of 122 cases was performed: 101 patients from the McGill University teaching hospitals and 21 patients from the Hillel Yaffe Medical center, Technion University. Patients included in the study were those with Bethesda V or VI thyroid nodules who underwent molecular testing (ThyGenext® or ThyroseqV3®) (McGill n = 72, Hillel Yaffe n = 14). Patients with Bethesda V or VI thyroid nodules who did not undergo molecular testing were used as controls (McGill n = 29, Hillel Yaffe n = 7). Each case was reviewed in order to determine whether the patient had optimal surgery. This was defined as total thyroidectomy in the presence of either a positive lymph node, extrathyroidal extension, or an aggressive pathological variant of papillary thyroid carcinoma (tall cell, hobnail, columnar cell, diffuse sclerosing, and solid/trabecular) documented on the final pathology report. In all other cases, a lobectomy/hemi/subtotal thyroidectomy was considered as optimal surgery. Chi-squared testing was performed to compare groups.</p><p><strong>Results: </strong>When molecular testing was done, 91.86% (79/86) of surgeries in the molecular testing group were optimal, compared to 61.11% (22/36) in the control group. At McGill University teaching hospitals and at Hillel Yaffe, 91.67% (66/72) and 92.86% (13/14) of surgeries in the intervention group were considered as optimal, respectively. This compares to 58.62% (17/29) at McGill and 71.43% (5/7) at Hillel Yaffe when molecular testing was not performed (p = .001, p = .186).</p><p><strong>Conclusions: </strong>In this study, molecular testing in Bethesda V and VI thyroid tumors significantly improved the likelihood of optimal surgery. Therefore, molecular testing may have an important role in optimizing surgical procedures performed in the setting of Bethesda V and VI thyroid nodules. Prospective studies with larger sample sizes are required to further investigate this finding.</p>\",\"PeriodicalId\":520683,\"journal\":{\"name\":\"Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale\",\"volume\":\" \",\"pages\":\"29\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2021-04-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s40463-021-00500-6\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40463-021-00500-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40463-021-00500-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
摘要
背景:分子检测已被用于细胞学上不确定的甲状腺结节(Bethesda III和IV),其中恶性肿瘤的风险为10-40%。然而,迄今为止,分子检测在细胞学上可疑或阳性的恶性甲状腺结节(Bethesda V和VI)中的作用一直存在争议。本研究的目的是确定在Bethesda V型和VI型甲状腺结节中进行分子检测的患者是否比未进行分子检测的患者更常进行最佳手术范围。方法:回顾性分析122例病例,其中101例来自麦吉尔大学教学医院,21例来自以色列理工大学Hillel Yaffe医学中心。纳入研究的患者为Bethesda V型或VI型甲状腺结节患者,并接受了分子检测(ThyGenext®或ThyroseqV3®)(McGill n = 72, Hillel Yaffe n = 14)。未进行分子检测的Bethesda V或VI型甲状腺结节患者作为对照组(McGill n = 29, Hillel Yaffe n = 7)。每个病例都进行了审查,以确定患者是否进行了最佳手术。这被定义为在最终病理报告中出现淋巴结阳性、甲状腺外展或甲状腺乳头状癌侵袭性病理变异(高细胞、鞋钉、柱状细胞、弥漫性硬化和实性/小梁)的情况下进行全甲状腺切除术。在所有其他病例中,肺叶切除术/半甲状腺切除术/甲状腺次全切除术被认为是最佳手术。组间比较采用卡方检验。结果:行分子检测时,分子检测组91.86%(79/86)手术最佳,对照组61.11%(22/36)手术最佳。在McGill大学教学医院和Hillel Yaffe医院,干预组分别有91.67%(66/72)和92.86%(13/14)的手术被认为是最佳的。相比之下,未进行分子检测时,McGill的这一比例为58.62% (17/29),Hillel Yaffe为71.43%(5/7)。001, p = .186)。结论:在本研究中,Bethesda V型和VI型甲状腺肿瘤的分子检测显著提高了最佳手术的可能性。因此,分子检测可能在优化Bethesda V型和VI型甲状腺结节的手术过程中发挥重要作用。需要更大样本量的前瞻性研究来进一步调查这一发现。
Molecular testing for cytologically suspicious and malignant (Bethesda V and VI) thyroid nodules to optimize the extent of surgical intervention: a retrospective chart review.
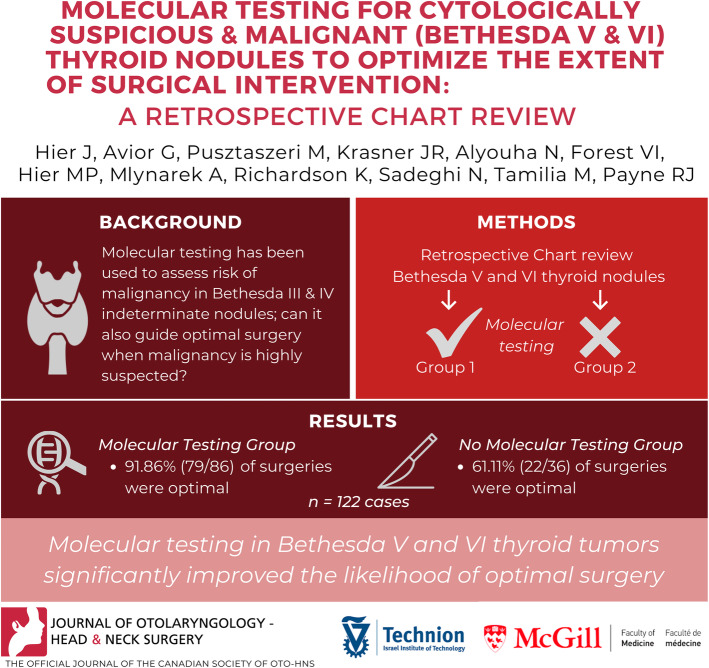
Background: Molecular testing has been used for cytologically indeterminate thyroid nodules (Bethesda III and IV), where the risk of malignancy is 10-40%. However, to date, the role of molecular testing in cytologically suspicious or positive for malignancy (Bethesda V and VI) thyroid nodules has been controversial. The aim of this study was to determine whether patients who had molecular testing in Bethesda V and VI thyroid nodules had the optimal extent of surgery performed more often than patients who did not have molecular testing performed.
Methods: A retrospective chart review of 122 cases was performed: 101 patients from the McGill University teaching hospitals and 21 patients from the Hillel Yaffe Medical center, Technion University. Patients included in the study were those with Bethesda V or VI thyroid nodules who underwent molecular testing (ThyGenext® or ThyroseqV3®) (McGill n = 72, Hillel Yaffe n = 14). Patients with Bethesda V or VI thyroid nodules who did not undergo molecular testing were used as controls (McGill n = 29, Hillel Yaffe n = 7). Each case was reviewed in order to determine whether the patient had optimal surgery. This was defined as total thyroidectomy in the presence of either a positive lymph node, extrathyroidal extension, or an aggressive pathological variant of papillary thyroid carcinoma (tall cell, hobnail, columnar cell, diffuse sclerosing, and solid/trabecular) documented on the final pathology report. In all other cases, a lobectomy/hemi/subtotal thyroidectomy was considered as optimal surgery. Chi-squared testing was performed to compare groups.
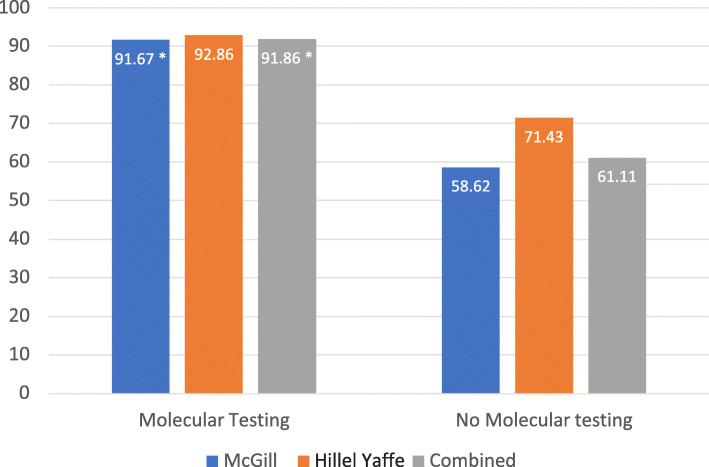
Results: When molecular testing was done, 91.86% (79/86) of surgeries in the molecular testing group were optimal, compared to 61.11% (22/36) in the control group. At McGill University teaching hospitals and at Hillel Yaffe, 91.67% (66/72) and 92.86% (13/14) of surgeries in the intervention group were considered as optimal, respectively. This compares to 58.62% (17/29) at McGill and 71.43% (5/7) at Hillel Yaffe when molecular testing was not performed (p = .001, p = .186).
Conclusions: In this study, molecular testing in Bethesda V and VI thyroid tumors significantly improved the likelihood of optimal surgery. Therefore, molecular testing may have an important role in optimizing surgical procedures performed in the setting of Bethesda V and VI thyroid nodules. Prospective studies with larger sample sizes are required to further investigate this finding.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


