Daria N Podlekareva, Dorte Bek Folkvardsen, Alena Skrahina, Anna Vassilenko, Aliaksandr Skrahin, Henadz Hurevich, Dzmitry Klimuk, Igor Karpov, Jens D Lundgren, Ole Kirk, Troels Lillebaek
{"title":"白俄罗斯 HIV 阳性肺结核患者的肺结核药物敏感性、治疗和结果:来自国家和国际实验室的结果。","authors":"Daria N Podlekareva, Dorte Bek Folkvardsen, Alena Skrahina, Anna Vassilenko, Aliaksandr Skrahin, Henadz Hurevich, Dzmitry Klimuk, Igor Karpov, Jens D Lundgren, Ole Kirk, Troels Lillebaek","doi":"10.1155/2021/6646239","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To cure drug-resistant (DR) tuberculosis (TB), the antituberculous treatment should be guided by <i>Mycobacterium tuberculosis</i> drug-susceptibility testing (DST). In this study, we compared conventional DST performed in Minsk, Belarus, a TB DR high-burden country, with extensive geno- and phenotypic analyses performed at the WHO TB Supranational Reference Laboratory in Copenhagen, Denmark, for TB/HIV coinfected patients. Subsequently, DST results were related to treatment regimen and outcome.</p><p><strong>Methods: </strong>Thirty TB/HIV coinfected patients from Minsk were included and descriptive statistics applied.</p><p><strong>Results: </strong>Based on results from Minsk, 10 (33%) TB/HIV patients had drug-sensitive TB. Two (7%) had isoniazid monoresistant TB, 8 (27%) had multidrug-resistant (MDR) TB, 5 (17%) preextensive drug-resistant (preXDR) TB, and 5 (17%) had extensive drug-resistant (XDR) TB. For the first-line drugs rifampicin and isoniazid, there was DST agreement between Minsk and Copenhagen for 90% patients. For the second-line anti-TB drugs, discrepancies were more pronounced. For 14 (47%) patients, there were disagreements for at least one drug, and 4 (13%) patients were classified as having MDR-TB in Minsk but were classified as having preXDR-TB based on DST results in Copenhagen. Initially, all patients received standard anti-TB treatment with rifampicin, isoniazid, pyrazinamide, and ethambutol. However, this was only suitable for 40% of the patients based on DST. On average, DR-TB patients were changed to 4 (IQR 3-5) active drugs after 1.5 months (IQR 1-2). After treatment adjustment, the treatment duration was 8 months (IQR 2-11). Four (22%) patients with DR-TB received treatment for >18 months. In total, sixteen (53%) patients died during 24 months of follow-up.</p><p><strong>Conclusions: </strong>We found high concordance for rifampicin and isoniazid DST between the Minsk and Copenhagen laboratories, whereas discrepancies for second-line drugs were more pronounced. For patients with DR-TB, treatment was often insufficient and relevant adjustments delayed. This example from Minsk, Belarus, underlines two crucial points in the management of DR-TB: the urgent need for implementation of rapid molecular DSTs and availability of second-line drugs in all DR-TB high-burden settings. Carefully designed individualized treatment regimens in accordance with DST patterns will likely improve patients' outcome and reduce transmission with drug-resistant <i>Mycobacterium tuberculosis</i> strains.</p>","PeriodicalId":30261,"journal":{"name":"Tuberculosis Research and Treatment","volume":"2021 ","pages":"6646239"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8035031/pdf/","citationCount":"0","resultStr":"{\"title\":\"Tuberculosis Drug Susceptibility, Treatment, and Outcomes for Belarusian HIV-Positive Patients with Tuberculosis: Results from a National and International Laboratory.\",\"authors\":\"Daria N Podlekareva, Dorte Bek Folkvardsen, Alena Skrahina, Anna Vassilenko, Aliaksandr Skrahin, Henadz Hurevich, Dzmitry Klimuk, Igor Karpov, Jens D Lundgren, Ole Kirk, Troels Lillebaek\",\"doi\":\"10.1155/2021/6646239\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To cure drug-resistant (DR) tuberculosis (TB), the antituberculous treatment should be guided by <i>Mycobacterium tuberculosis</i> drug-susceptibility testing (DST). In this study, we compared conventional DST performed in Minsk, Belarus, a TB DR high-burden country, with extensive geno- and phenotypic analyses performed at the WHO TB Supranational Reference Laboratory in Copenhagen, Denmark, for TB/HIV coinfected patients. Subsequently, DST results were related to treatment regimen and outcome.</p><p><strong>Methods: </strong>Thirty TB/HIV coinfected patients from Minsk were included and descriptive statistics applied.</p><p><strong>Results: </strong>Based on results from Minsk, 10 (33%) TB/HIV patients had drug-sensitive TB. Two (7%) had isoniazid monoresistant TB, 8 (27%) had multidrug-resistant (MDR) TB, 5 (17%) preextensive drug-resistant (preXDR) TB, and 5 (17%) had extensive drug-resistant (XDR) TB. For the first-line drugs rifampicin and isoniazid, there was DST agreement between Minsk and Copenhagen for 90% patients. For the second-line anti-TB drugs, discrepancies were more pronounced. For 14 (47%) patients, there were disagreements for at least one drug, and 4 (13%) patients were classified as having MDR-TB in Minsk but were classified as having preXDR-TB based on DST results in Copenhagen. Initially, all patients received standard anti-TB treatment with rifampicin, isoniazid, pyrazinamide, and ethambutol. However, this was only suitable for 40% of the patients based on DST. On average, DR-TB patients were changed to 4 (IQR 3-5) active drugs after 1.5 months (IQR 1-2). After treatment adjustment, the treatment duration was 8 months (IQR 2-11). Four (22%) patients with DR-TB received treatment for >18 months. In total, sixteen (53%) patients died during 24 months of follow-up.</p><p><strong>Conclusions: </strong>We found high concordance for rifampicin and isoniazid DST between the Minsk and Copenhagen laboratories, whereas discrepancies for second-line drugs were more pronounced. For patients with DR-TB, treatment was often insufficient and relevant adjustments delayed. This example from Minsk, Belarus, underlines two crucial points in the management of DR-TB: the urgent need for implementation of rapid molecular DSTs and availability of second-line drugs in all DR-TB high-burden settings. Carefully designed individualized treatment regimens in accordance with DST patterns will likely improve patients' outcome and reduce transmission with drug-resistant <i>Mycobacterium tuberculosis</i> strains.</p>\",\"PeriodicalId\":30261,\"journal\":{\"name\":\"Tuberculosis Research and Treatment\",\"volume\":\"2021 \",\"pages\":\"6646239\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8035031/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tuberculosis Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/6646239\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberculosis Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/6646239","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Tuberculosis Drug Susceptibility, Treatment, and Outcomes for Belarusian HIV-Positive Patients with Tuberculosis: Results from a National and International Laboratory.
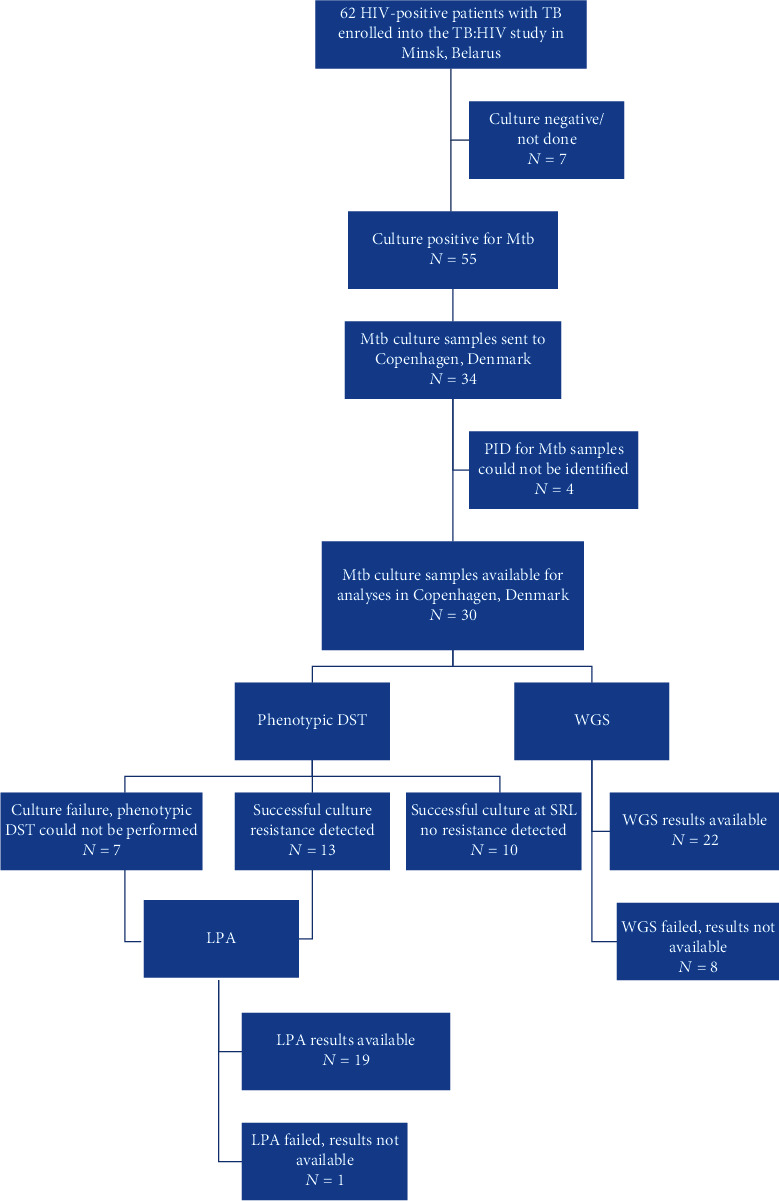
Background: To cure drug-resistant (DR) tuberculosis (TB), the antituberculous treatment should be guided by Mycobacterium tuberculosis drug-susceptibility testing (DST). In this study, we compared conventional DST performed in Minsk, Belarus, a TB DR high-burden country, with extensive geno- and phenotypic analyses performed at the WHO TB Supranational Reference Laboratory in Copenhagen, Denmark, for TB/HIV coinfected patients. Subsequently, DST results were related to treatment regimen and outcome.
Methods: Thirty TB/HIV coinfected patients from Minsk were included and descriptive statistics applied.
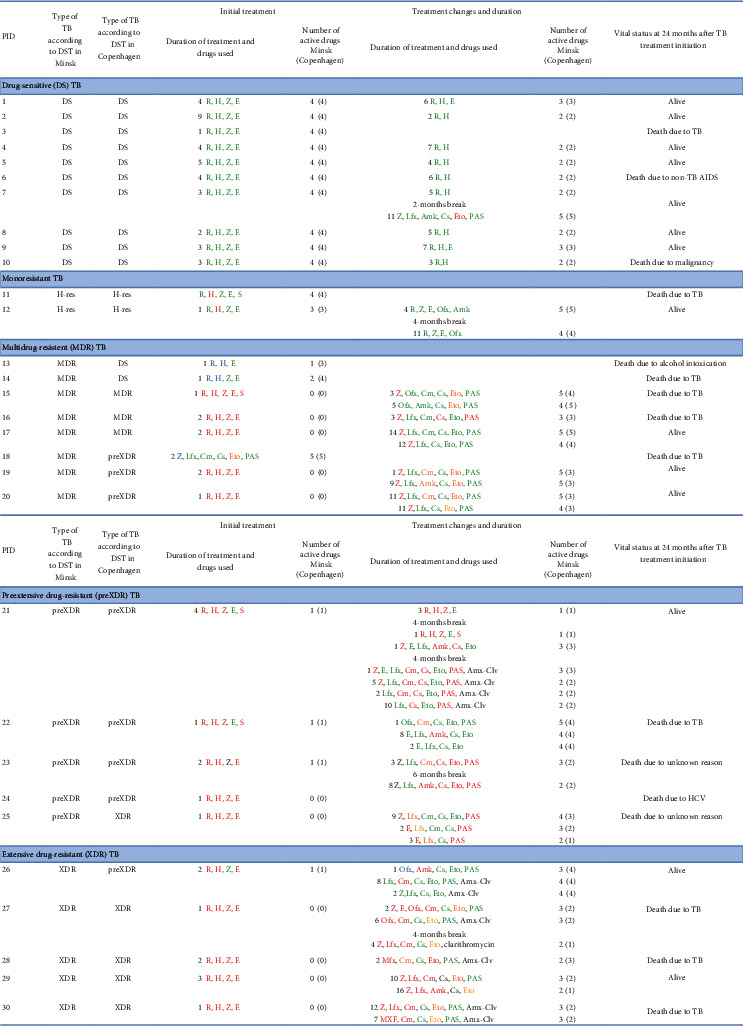
Results: Based on results from Minsk, 10 (33%) TB/HIV patients had drug-sensitive TB. Two (7%) had isoniazid monoresistant TB, 8 (27%) had multidrug-resistant (MDR) TB, 5 (17%) preextensive drug-resistant (preXDR) TB, and 5 (17%) had extensive drug-resistant (XDR) TB. For the first-line drugs rifampicin and isoniazid, there was DST agreement between Minsk and Copenhagen for 90% patients. For the second-line anti-TB drugs, discrepancies were more pronounced. For 14 (47%) patients, there were disagreements for at least one drug, and 4 (13%) patients were classified as having MDR-TB in Minsk but were classified as having preXDR-TB based on DST results in Copenhagen. Initially, all patients received standard anti-TB treatment with rifampicin, isoniazid, pyrazinamide, and ethambutol. However, this was only suitable for 40% of the patients based on DST. On average, DR-TB patients were changed to 4 (IQR 3-5) active drugs after 1.5 months (IQR 1-2). After treatment adjustment, the treatment duration was 8 months (IQR 2-11). Four (22%) patients with DR-TB received treatment for >18 months. In total, sixteen (53%) patients died during 24 months of follow-up.
Conclusions: We found high concordance for rifampicin and isoniazid DST between the Minsk and Copenhagen laboratories, whereas discrepancies for second-line drugs were more pronounced. For patients with DR-TB, treatment was often insufficient and relevant adjustments delayed. This example from Minsk, Belarus, underlines two crucial points in the management of DR-TB: the urgent need for implementation of rapid molecular DSTs and availability of second-line drugs in all DR-TB high-burden settings. Carefully designed individualized treatment regimens in accordance with DST patterns will likely improve patients' outcome and reduce transmission with drug-resistant Mycobacterium tuberculosis strains.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


