Biggie Baffour-Awuah , Gudrun Dieberg , Melissa J. Pearson , Neil A. Smart
{"title":"老年高血压患者的血压控制:荟萃分析和荟萃回归的系统综述","authors":"Biggie Baffour-Awuah , Gudrun Dieberg , Melissa J. Pearson , Neil A. Smart","doi":"10.1016/j.ijchy.2020.100040","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Managing blood pressure reduces CVD risk, but optimal treatment thresholds remain unclear as it is a balancing act to avoid hypotension-related adverse events.</p></div><div><h3>Objectives</h3><p>This systematic review, meta-analysis and meta-regression evaluated the benefits of intensive BP treatment in hypertensive older adults.</p></div><div><h3>Methods</h3><p>We systematically searched PubMed, MEDLINE, EMBASE, and the Cochrane Library of Controlled Trials until January 31, 2020. Studies comparing different BP treatments/targets and/or active BP against placebo treatment, with a minimum 12 months follow-up, were included. Risk ratios (RR) and 95% CIs were calculated using a random effects model. The primary outcome was RR of major cardiovascular events (MCEs); secondary outcomes included myocardial infarction (MI), stroke, heart failure (HF), cardiovascular (CV) mortality, and all-cause mortality.</p></div><div><h3>Results</h3><p>We included 16 studies totaling 65,890 hypertensive participants (average age 69.4 years) with a follow-up period from 1.8 to 4.9 years. Intensive BP treatment significantly reduced the relative risk of MCEs by 26% (RR:0.74, 95%CI 0.64–0.86, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 79.71%). RR of MI significantly reduced by 13% (RR:0.87, 95%CI 0.76–1.00, <em>p</em> = 0.052; <em>I</em><sup>2</sup> = 0.00%), stroke by 28% (RR:0.72, 95%CI 0.64–0.82, <em>p</em> = 0.000; <em>I</em><sup><em>2</em></sup> = 32.45%), HF by 47% (RR:0.53, 95% CI 0.43–0.66, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 1.23%), and CV mortality by 24% (RR:0.76, 95%CI 0.66–0.89, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 39.74%). All-cause mortality reduced by 17% (RR:0.83, 95%CI 0.73–0.93, <em>p</em> = 0.001; <em>I</em><sup>2</sup> = 53.09%). Of the participants - 61% reached BP targets and 5% withdrew; with 1 hypotension-related event per 780 people treated.</p></div><div><h3>Conclusions</h3><p>Lower BP treatment targets are optimal for CV protection, effective, well-tolerated and safe, and support the latest hypertension guidelines.</p></div>","PeriodicalId":36839,"journal":{"name":"International Journal of Cardiology: Hypertension","volume":"6 ","pages":"Article 100040"},"PeriodicalIF":0.0000,"publicationDate":"2020-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchy.2020.100040","citationCount":"8","resultStr":"{\"title\":\"Blood pressure control in older adults with hypertension: A systematic review with meta-analysis and meta-regression\",\"authors\":\"Biggie Baffour-Awuah , Gudrun Dieberg , Melissa J. Pearson , Neil A. Smart\",\"doi\":\"10.1016/j.ijchy.2020.100040\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Managing blood pressure reduces CVD risk, but optimal treatment thresholds remain unclear as it is a balancing act to avoid hypotension-related adverse events.</p></div><div><h3>Objectives</h3><p>This systematic review, meta-analysis and meta-regression evaluated the benefits of intensive BP treatment in hypertensive older adults.</p></div><div><h3>Methods</h3><p>We systematically searched PubMed, MEDLINE, EMBASE, and the Cochrane Library of Controlled Trials until January 31, 2020. Studies comparing different BP treatments/targets and/or active BP against placebo treatment, with a minimum 12 months follow-up, were included. Risk ratios (RR) and 95% CIs were calculated using a random effects model. The primary outcome was RR of major cardiovascular events (MCEs); secondary outcomes included myocardial infarction (MI), stroke, heart failure (HF), cardiovascular (CV) mortality, and all-cause mortality.</p></div><div><h3>Results</h3><p>We included 16 studies totaling 65,890 hypertensive participants (average age 69.4 years) with a follow-up period from 1.8 to 4.9 years. Intensive BP treatment significantly reduced the relative risk of MCEs by 26% (RR:0.74, 95%CI 0.64–0.86, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 79.71%). RR of MI significantly reduced by 13% (RR:0.87, 95%CI 0.76–1.00, <em>p</em> = 0.052; <em>I</em><sup>2</sup> = 0.00%), stroke by 28% (RR:0.72, 95%CI 0.64–0.82, <em>p</em> = 0.000; <em>I</em><sup><em>2</em></sup> = 32.45%), HF by 47% (RR:0.53, 95% CI 0.43–0.66, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 1.23%), and CV mortality by 24% (RR:0.76, 95%CI 0.66–0.89, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 39.74%). All-cause mortality reduced by 17% (RR:0.83, 95%CI 0.73–0.93, <em>p</em> = 0.001; <em>I</em><sup>2</sup> = 53.09%). Of the participants - 61% reached BP targets and 5% withdrew; with 1 hypotension-related event per 780 people treated.</p></div><div><h3>Conclusions</h3><p>Lower BP treatment targets are optimal for CV protection, effective, well-tolerated and safe, and support the latest hypertension guidelines.</p></div>\",\"PeriodicalId\":36839,\"journal\":{\"name\":\"International Journal of Cardiology: Hypertension\",\"volume\":\"6 \",\"pages\":\"Article 100040\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.ijchy.2020.100040\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Cardiology: Hypertension\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590086220300173\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiology: Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590086220300173","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 8
摘要
控制血压可降低心血管疾病风险,但最佳治疗阈值仍不清楚,因为它是避免低血压相关不良事件的平衡行为。目的:本系统综述、荟萃分析和荟萃回归评估强化血压治疗对老年人高血压的益处。方法系统检索PubMed、MEDLINE、EMBASE和Cochrane对照试验库,检索截止日期为2020年1月31日。比较不同的BP治疗/靶点和/或活性BP与安慰剂治疗的研究,至少随访12个月。采用随机效应模型计算风险比(RR)和95% ci。主要终点为主要心血管事件(MCEs)的RR;次要结局包括心肌梗死(MI)、中风、心力衰竭(HF)、心血管(CV)死亡率和全因死亡率。结果我们纳入了16项研究,共65,890名高血压患者(平均年龄69.4岁),随访时间为1.8至4.9年。强化降压治疗可显著降低mce的相对风险26% (RR:0.74, 95%CI 0.64-0.86, p = 0.000;i2 = 79.71%)。MI的RR显著降低13% (RR:0.87, 95%CI 0.76-1.00, p = 0.052;I2 = 0.00%), 28%的中风(RR: 0.72, 95% ci 0.64 - -0.82, p = 0.000;I2 = 32.45%),高频47% (RR: 0.53, 95% CI 0.43 - -0.66, p = 0.000;I2 = 1.23%), CV死亡率降低24% (RR:0.76, 95%CI 0.66-0.89, p = 0.000;i2 = 39.74%)。全因死亡率降低17% (RR:0.83, 95%CI 0.73-0.93, p = 0.001;i2 = 53.09%)。在参与者中,61%达到了BP目标,5%退出;每780名接受治疗的患者中有1例低血压相关事件。结论慢速降压治疗目标对心血管保护效果最佳,有效、耐受性好、安全,支持最新高血压指南。
Blood pressure control in older adults with hypertension: A systematic review with meta-analysis and meta-regression
Background
Managing blood pressure reduces CVD risk, but optimal treatment thresholds remain unclear as it is a balancing act to avoid hypotension-related adverse events.
Objectives
This systematic review, meta-analysis and meta-regression evaluated the benefits of intensive BP treatment in hypertensive older adults.
Methods
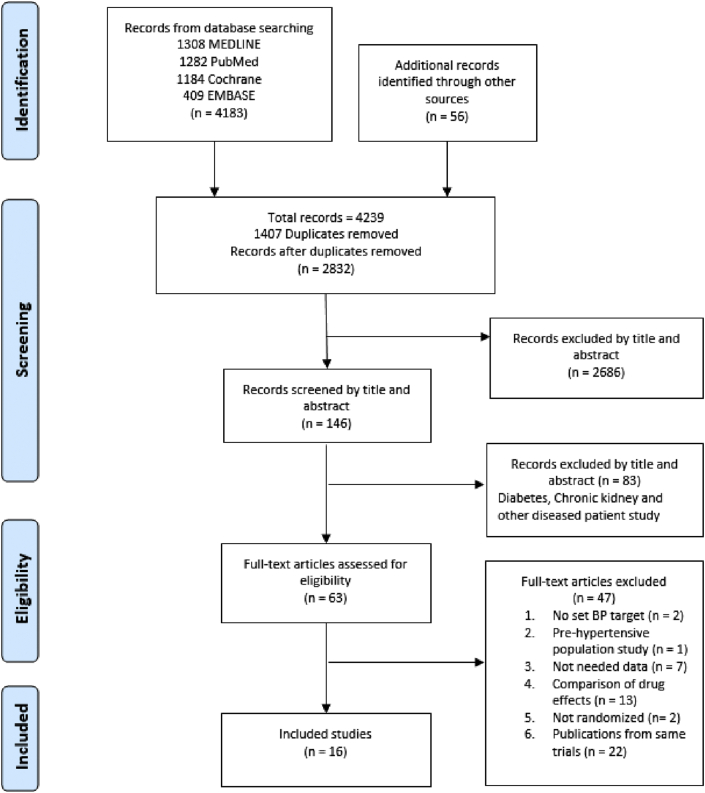
We systematically searched PubMed, MEDLINE, EMBASE, and the Cochrane Library of Controlled Trials until January 31, 2020. Studies comparing different BP treatments/targets and/or active BP against placebo treatment, with a minimum 12 months follow-up, were included. Risk ratios (RR) and 95% CIs were calculated using a random effects model. The primary outcome was RR of major cardiovascular events (MCEs); secondary outcomes included myocardial infarction (MI), stroke, heart failure (HF), cardiovascular (CV) mortality, and all-cause mortality.
Results
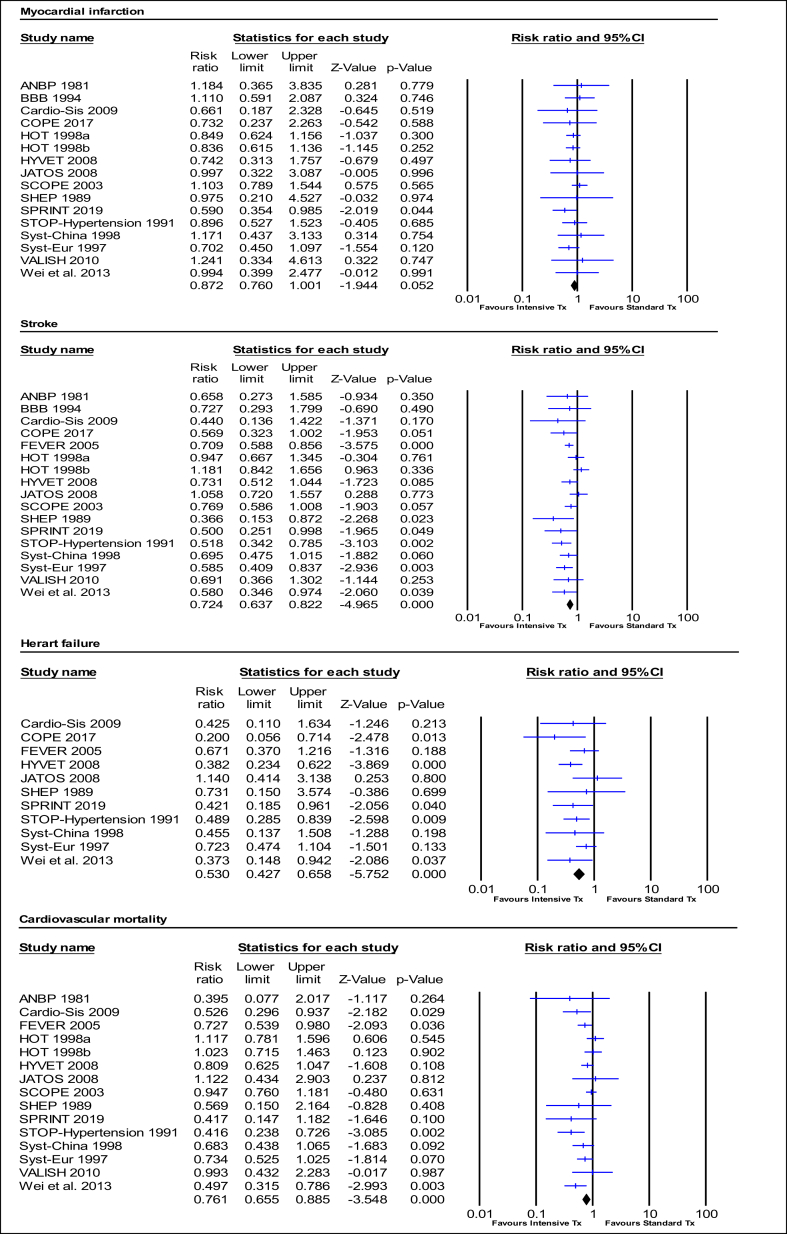
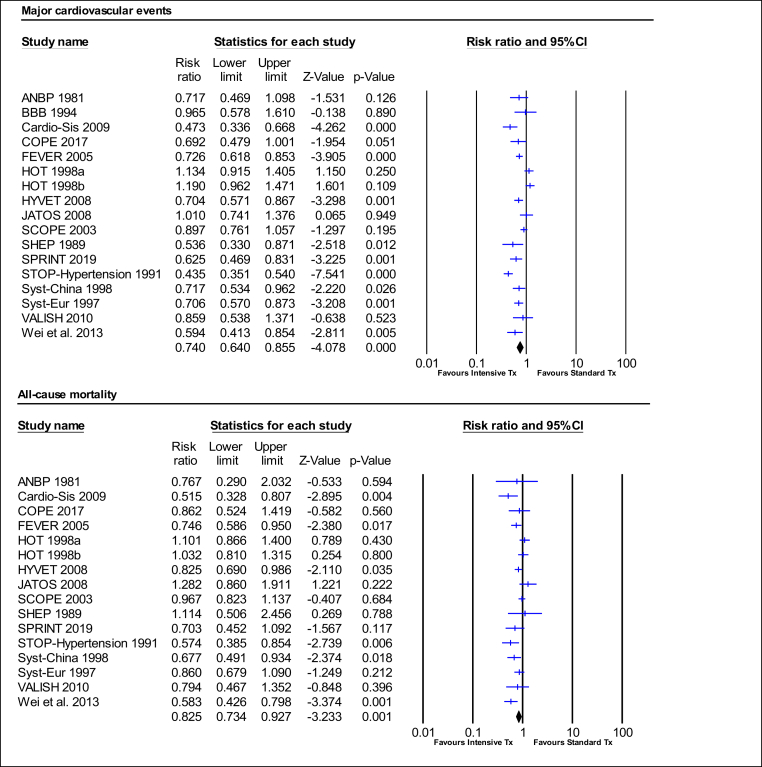
We included 16 studies totaling 65,890 hypertensive participants (average age 69.4 years) with a follow-up period from 1.8 to 4.9 years. Intensive BP treatment significantly reduced the relative risk of MCEs by 26% (RR:0.74, 95%CI 0.64–0.86, p = 0.000; I2 = 79.71%). RR of MI significantly reduced by 13% (RR:0.87, 95%CI 0.76–1.00, p = 0.052; I2 = 0.00%), stroke by 28% (RR:0.72, 95%CI 0.64–0.82, p = 0.000; I2 = 32.45%), HF by 47% (RR:0.53, 95% CI 0.43–0.66, p = 0.000; I2 = 1.23%), and CV mortality by 24% (RR:0.76, 95%CI 0.66–0.89, p = 0.000; I2 = 39.74%). All-cause mortality reduced by 17% (RR:0.83, 95%CI 0.73–0.93, p = 0.001; I2 = 53.09%). Of the participants - 61% reached BP targets and 5% withdrew; with 1 hypotension-related event per 780 people treated.
Conclusions
Lower BP treatment targets are optimal for CV protection, effective, well-tolerated and safe, and support the latest hypertension guidelines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


