Mary Dooley, Annie N Simpson, Paul J Nietert, Dunc Williams, Kit N Simpson
{"title":"成本节约的最小差异:是否有可能确定成本节约的MID ?","authors":"Mary Dooley, Annie N Simpson, Paul J Nietert, Dunc Williams, Kit N Simpson","doi":"10.1007/s10742-020-00233-5","DOIUrl":null,"url":null,"abstract":"<p><p>As healthcare costs continue to increase, studies assessing costs are becoming increasingly common, but researchers planning for studies that measure costs differences (savings) encounter a lack of literature or consensus among researchers on what constitutes \"small\" or \"large\" cost savings for common measures of resource use. Other fields of research have developed approaches to solve this type of problem. Researchers measuring improvement in quality of life or clinical assessments have defined minimally important differences (MID) which are then used to define magnitudes when planning studies. Also, studies that measure cost effectiveness use benchmarks, such as cost/QALY, but do not provide benchmarks for cost differences. In a review of the literature, we found no publications identifying indicators of magnitude for costs. However, the literature describes three approaches used to identify minimally important outcome differences: (1) anchor-based, (2) distribution-based, and (3) a consensus-based Delphi methods. In this exploratory study, we used these three approaches to derive MID for two types of resource measures common in costing studies for: (1) hospital admissions (high cost); and (2) clinic visits (low cost). We used data from two (unpublished) studies to implement the MID estimation. Because the distributional characteristics of cost measures may require substantial samples, we performed power analyses on all our estimates to illustrate the effect that the definitions of \"small\" and \"large\" costs may be expected to have on power and sample size requirements for studies. The anchor-based method, while logical and simple to implement, may be of limited value in cases where it is difficult to identify appropriate anchors. We observed some commonalities and differences for the distribution and consensus-based approaches, which require further examination. We recommend that in cases where acceptable anchors are not available, both the Delphi and the distribution-method of MID for costs be explored for convergence.</p>","PeriodicalId":45600,"journal":{"name":"Health Services and Outcomes Research Methodology","volume":"21 1","pages":"131-144"},"PeriodicalIF":1.6000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s10742-020-00233-5","citationCount":"5","resultStr":"{\"title\":\"Minimally important difference in cost savings: Is it possible to identify an MID for cost savings?\",\"authors\":\"Mary Dooley, Annie N Simpson, Paul J Nietert, Dunc Williams, Kit N Simpson\",\"doi\":\"10.1007/s10742-020-00233-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>As healthcare costs continue to increase, studies assessing costs are becoming increasingly common, but researchers planning for studies that measure costs differences (savings) encounter a lack of literature or consensus among researchers on what constitutes \\\"small\\\" or \\\"large\\\" cost savings for common measures of resource use. Other fields of research have developed approaches to solve this type of problem. Researchers measuring improvement in quality of life or clinical assessments have defined minimally important differences (MID) which are then used to define magnitudes when planning studies. Also, studies that measure cost effectiveness use benchmarks, such as cost/QALY, but do not provide benchmarks for cost differences. In a review of the literature, we found no publications identifying indicators of magnitude for costs. However, the literature describes three approaches used to identify minimally important outcome differences: (1) anchor-based, (2) distribution-based, and (3) a consensus-based Delphi methods. In this exploratory study, we used these three approaches to derive MID for two types of resource measures common in costing studies for: (1) hospital admissions (high cost); and (2) clinic visits (low cost). We used data from two (unpublished) studies to implement the MID estimation. Because the distributional characteristics of cost measures may require substantial samples, we performed power analyses on all our estimates to illustrate the effect that the definitions of \\\"small\\\" and \\\"large\\\" costs may be expected to have on power and sample size requirements for studies. The anchor-based method, while logical and simple to implement, may be of limited value in cases where it is difficult to identify appropriate anchors. We observed some commonalities and differences for the distribution and consensus-based approaches, which require further examination. We recommend that in cases where acceptable anchors are not available, both the Delphi and the distribution-method of MID for costs be explored for convergence.</p>\",\"PeriodicalId\":45600,\"journal\":{\"name\":\"Health Services and Outcomes Research Methodology\",\"volume\":\"21 1\",\"pages\":\"131-144\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1007/s10742-020-00233-5\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Services and Outcomes Research Methodology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s10742-020-00233-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services and Outcomes Research Methodology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10742-020-00233-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Minimally important difference in cost savings: Is it possible to identify an MID for cost savings?
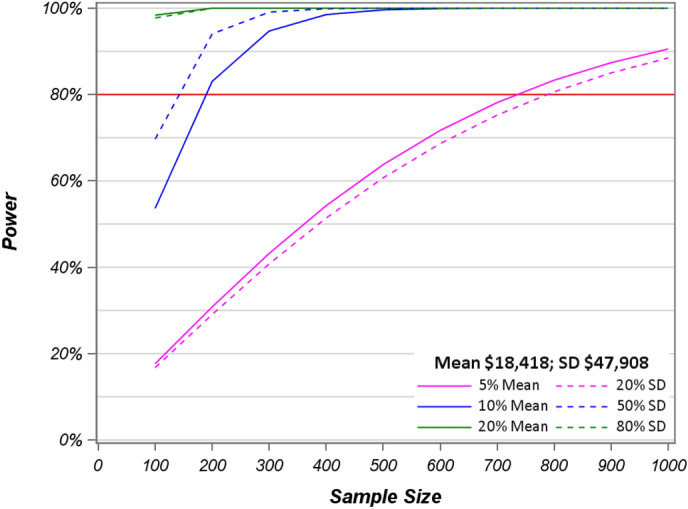
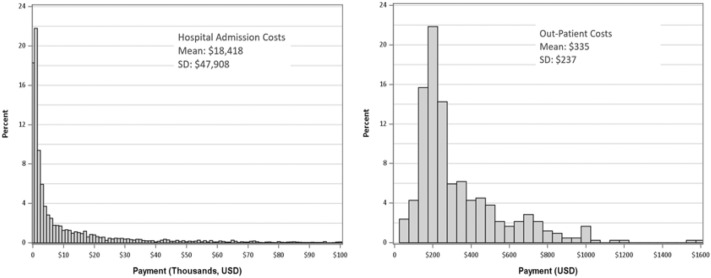
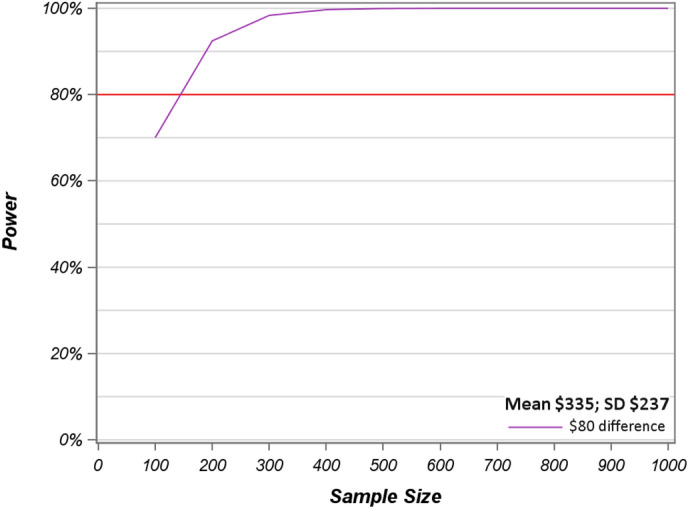
As healthcare costs continue to increase, studies assessing costs are becoming increasingly common, but researchers planning for studies that measure costs differences (savings) encounter a lack of literature or consensus among researchers on what constitutes "small" or "large" cost savings for common measures of resource use. Other fields of research have developed approaches to solve this type of problem. Researchers measuring improvement in quality of life or clinical assessments have defined minimally important differences (MID) which are then used to define magnitudes when planning studies. Also, studies that measure cost effectiveness use benchmarks, such as cost/QALY, but do not provide benchmarks for cost differences. In a review of the literature, we found no publications identifying indicators of magnitude for costs. However, the literature describes three approaches used to identify minimally important outcome differences: (1) anchor-based, (2) distribution-based, and (3) a consensus-based Delphi methods. In this exploratory study, we used these three approaches to derive MID for two types of resource measures common in costing studies for: (1) hospital admissions (high cost); and (2) clinic visits (low cost). We used data from two (unpublished) studies to implement the MID estimation. Because the distributional characteristics of cost measures may require substantial samples, we performed power analyses on all our estimates to illustrate the effect that the definitions of "small" and "large" costs may be expected to have on power and sample size requirements for studies. The anchor-based method, while logical and simple to implement, may be of limited value in cases where it is difficult to identify appropriate anchors. We observed some commonalities and differences for the distribution and consensus-based approaches, which require further examination. We recommend that in cases where acceptable anchors are not available, both the Delphi and the distribution-method of MID for costs be explored for convergence.
期刊介绍:
The journal reflects the multidisciplinary nature of the field of health services and outcomes research. It addresses the needs of multiple, interlocking communities, including methodologists in statistics, econometrics, social and behavioral sciences; designers and analysts of health policy and health services research projects; and health care providers and policy makers who need to properly understand and evaluate the results of published research. The journal strives to enhance the level of methodologic rigor in health services and outcomes research and contributes to the development of methodologic standards in the field. In pursuing its main objective, the journal also provides a meeting ground for researchers from a number of traditional disciplines and fosters the development of new quantitative, qualitative, and mixed methods by statisticians, econometricians, health services researchers, and methodologists in other fields. Health Services and Outcomes Research Methodology publishes: Research papers on quantitative, qualitative, and mixed methods; Case Studies describing applications of quantitative and qualitative methodology in health services and outcomes research; Review Articles synthesizing and popularizing methodologic developments; Tutorials; Articles on computational issues and software reviews; Book reviews; and Notices. Special issues will be devoted to papers presented at important workshops and conferences.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


