{"title":"协作质量改进对印度泰伦甘纳邦和安得拉邦医院死产、新生儿死亡率和新生儿护理实践的影响:来自准实验混合方法研究的证据。","authors":"Karen Zamboni, Samiksha Singh, Mukta Tyagi, Zelee Hill, Claudia Hanson, Joanna Schellenberg","doi":"10.1186/s13012-020-01058-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Improving quality of care is a key priority to reduce neonatal mortality and stillbirths. The Safe Care, Saving Lives programme aimed to improve care in newborn care units and labour wards of 60 public and private hospitals in Telangana and Andhra Pradesh, India, using a collaborative quality improvement approach. Our external evaluation of this programme aimed to evaluate programme effects on implementation of maternal and newborn care practices, and impact on stillbirths, 7- and 28-day neonatal mortality rate in labour wards and neonatal care units. We also aimed to evaluate programme implementation and mechanisms of change.</p><p><strong>Methods: </strong>We used a quasi-experimental plausibility design with a nested process evaluation. We evaluated effects on stillbirths, mortality and secondary outcomes relating to adherence to 20 evidence-based intrapartum and newborn care practices, comparing survey data from 29 hospitals receiving the intervention to 31 hospitals expected to receive the intervention later, using a difference-in-difference analysis. We analysed programme implementation data and conducted 42 semi-structured interviews in four case studies to describe implementation and address four theory-driven questions to explain the quantitative results.</p><p><strong>Results: </strong>Only 7 of the 29 intervention hospitals were engaged in the intervention for its entire duration. There was no evidence of an effect of the intervention on stillbirths [DiD - 1.3 percentage points, 95% CI - 2.6-0.1], on neonatal mortality at age 7 days [DiD - 1.6, 95% CI - 9-6.2] or 28 days [DiD - 3.0, 95% CI - 12.9-6.9] or on adherence to target evidence-based intrapartum and newborn care practices. The process evaluation identified challenges in engaging leaders; challenges in developing capacity for quality improvement; and challenges in activating mechanisms of change at the unit level, rather than for a few individuals, and in sustaining these through the creation of new social norms.</p><p><strong>Conclusion: </strong>Despite careful planning and substantial resources, the intervention was not feasible for implementation on a large scale. Greater focus is required on strategies to engage leadership. Quality improvement may need to be accompanied by clinical training. Further research is also needed on quality improvement using a health systems perspective.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"4"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13012-020-01058-z","citationCount":"14","resultStr":"{\"title\":\"Effect of collaborative quality improvement on stillbirths, neonatal mortality and newborn care practices in hospitals of Telangana and Andhra Pradesh, India: evidence from a quasi-experimental mixed-methods study.\",\"authors\":\"Karen Zamboni, Samiksha Singh, Mukta Tyagi, Zelee Hill, Claudia Hanson, Joanna Schellenberg\",\"doi\":\"10.1186/s13012-020-01058-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Improving quality of care is a key priority to reduce neonatal mortality and stillbirths. The Safe Care, Saving Lives programme aimed to improve care in newborn care units and labour wards of 60 public and private hospitals in Telangana and Andhra Pradesh, India, using a collaborative quality improvement approach. Our external evaluation of this programme aimed to evaluate programme effects on implementation of maternal and newborn care practices, and impact on stillbirths, 7- and 28-day neonatal mortality rate in labour wards and neonatal care units. We also aimed to evaluate programme implementation and mechanisms of change.</p><p><strong>Methods: </strong>We used a quasi-experimental plausibility design with a nested process evaluation. We evaluated effects on stillbirths, mortality and secondary outcomes relating to adherence to 20 evidence-based intrapartum and newborn care practices, comparing survey data from 29 hospitals receiving the intervention to 31 hospitals expected to receive the intervention later, using a difference-in-difference analysis. We analysed programme implementation data and conducted 42 semi-structured interviews in four case studies to describe implementation and address four theory-driven questions to explain the quantitative results.</p><p><strong>Results: </strong>Only 7 of the 29 intervention hospitals were engaged in the intervention for its entire duration. There was no evidence of an effect of the intervention on stillbirths [DiD - 1.3 percentage points, 95% CI - 2.6-0.1], on neonatal mortality at age 7 days [DiD - 1.6, 95% CI - 9-6.2] or 28 days [DiD - 3.0, 95% CI - 12.9-6.9] or on adherence to target evidence-based intrapartum and newborn care practices. The process evaluation identified challenges in engaging leaders; challenges in developing capacity for quality improvement; and challenges in activating mechanisms of change at the unit level, rather than for a few individuals, and in sustaining these through the creation of new social norms.</p><p><strong>Conclusion: </strong>Despite careful planning and substantial resources, the intervention was not feasible for implementation on a large scale. Greater focus is required on strategies to engage leadership. Quality improvement may need to be accompanied by clinical training. Further research is also needed on quality improvement using a health systems perspective.</p>\",\"PeriodicalId\":417097,\"journal\":{\"name\":\"Implementation Science : IS\",\"volume\":\" \",\"pages\":\"4\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13012-020-01058-z\",\"citationCount\":\"14\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation Science : IS\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13012-020-01058-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13012-020-01058-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 14
摘要
背景:提高护理质量是降低新生儿死亡率和死产的关键优先事项。“安全护理,拯救生命”方案旨在通过协作提高质量的方法,改善印度特伦甘纳邦和安得拉邦60家公立和私立医院新生儿护理室和产房的护理。我们对该方案的外部评估旨在评估该方案对孕产妇和新生儿护理实践实施的影响,以及对产房和新生儿护理病房死胎、7天和28天新生儿死亡率的影响。我们还旨在评估方案执行情况和变革机制。方法:采用准实验似然设计,嵌套工艺评价。我们评估了与坚持20种循证分娩和新生儿护理实践有关的死产、死亡率和次要结局的影响,比较了29家接受干预的医院和31家预计将接受干预的医院的调查数据,采用差异中差异分析。我们分析了项目实施数据,并在四个案例研究中进行了42次半结构化访谈,以描述实施情况并解决四个理论驱动的问题,以解释定量结果。结果:29家干预医院中仅有7家全程参与干预。没有证据表明干预对死产的影响[DiD - 1.3个百分点,95% CI - 2.6-0.1],对7天新生儿死亡率[DiD - 1.6, 95% CI - 9-6.2]或28天新生儿死亡率[DiD - 3.0, 95% CI - 12.9-6.9]或对目标循证分娩和新生儿护理实践的影响。过程评估确定了吸引领导者的挑战;发展质量改进能力的挑战;以及在单位层面上激活变革机制的挑战,而不是针对少数个人,并通过创造新的社会规范来维持这些机制。结论:尽管经过精心规划和大量资源,该干预措施仍不可行,无法大规模实施。需要更多地关注吸引领导层参与的战略。质量改进可能需要伴随临床培训。还需要从卫生系统的角度对质量改进进行进一步研究。
Effect of collaborative quality improvement on stillbirths, neonatal mortality and newborn care practices in hospitals of Telangana and Andhra Pradesh, India: evidence from a quasi-experimental mixed-methods study.
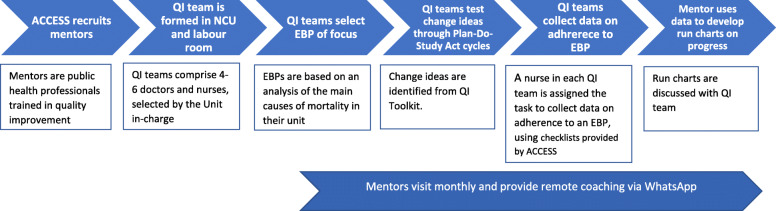
Background: Improving quality of care is a key priority to reduce neonatal mortality and stillbirths. The Safe Care, Saving Lives programme aimed to improve care in newborn care units and labour wards of 60 public and private hospitals in Telangana and Andhra Pradesh, India, using a collaborative quality improvement approach. Our external evaluation of this programme aimed to evaluate programme effects on implementation of maternal and newborn care practices, and impact on stillbirths, 7- and 28-day neonatal mortality rate in labour wards and neonatal care units. We also aimed to evaluate programme implementation and mechanisms of change.
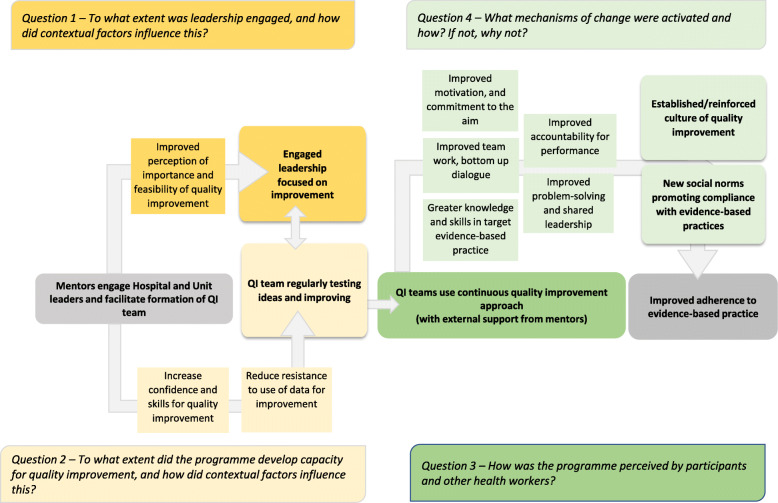
Methods: We used a quasi-experimental plausibility design with a nested process evaluation. We evaluated effects on stillbirths, mortality and secondary outcomes relating to adherence to 20 evidence-based intrapartum and newborn care practices, comparing survey data from 29 hospitals receiving the intervention to 31 hospitals expected to receive the intervention later, using a difference-in-difference analysis. We analysed programme implementation data and conducted 42 semi-structured interviews in four case studies to describe implementation and address four theory-driven questions to explain the quantitative results.
Results: Only 7 of the 29 intervention hospitals were engaged in the intervention for its entire duration. There was no evidence of an effect of the intervention on stillbirths [DiD - 1.3 percentage points, 95% CI - 2.6-0.1], on neonatal mortality at age 7 days [DiD - 1.6, 95% CI - 9-6.2] or 28 days [DiD - 3.0, 95% CI - 12.9-6.9] or on adherence to target evidence-based intrapartum and newborn care practices. The process evaluation identified challenges in engaging leaders; challenges in developing capacity for quality improvement; and challenges in activating mechanisms of change at the unit level, rather than for a few individuals, and in sustaining these through the creation of new social norms.
Conclusion: Despite careful planning and substantial resources, the intervention was not feasible for implementation on a large scale. Greater focus is required on strategies to engage leadership. Quality improvement may need to be accompanied by clinical training. Further research is also needed on quality improvement using a health systems perspective.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


