Heidi A Rantala, Sirpa Leivo-Korpela, Siiri Kettunen, Juho T Lehto, Lauri Lehtimäki
{"title":"长期无创通气受试者的生存和临终方面。","authors":"Heidi A Rantala, Sirpa Leivo-Korpela, Siiri Kettunen, Juho T Lehto, Lauri Lehtimäki","doi":"10.1080/20018525.2020.1840494","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The need for noninvasive ventilation (NIV) is commonly considered a predictor of poor survival, but life expectancy may vary depending on the underlying disease. We studied the factors associated with decreased survival and end-of-life characteristics in an unselected population of subjects starting NIV.</p><p><strong>Methods: </strong>We conducted a retrospective study including 205 subjects initiating NIV from 1/1/2012-31/12/2015 who were followed up until 31/12/2017.</p><p><strong>Results: </strong>The median survival time was shorter in subjects needing help with activities of daily living than in independent subjects (hazard ratio (HR) for death 1.7, 95% CI 1.2-2.6, <i>P</i> = 0.008) and was also shorter in subjects on long-term oxygen therapy (LTOT) than in those not on LTOT (HR for death 2.8, 95% CI 1.9-4.3, <i>P</i> < 0.001). There was marked difference in survival according to the disease necessitating NIV, and subjects with amyotrophic lateral sclerosis or interstitial lung disease seemed to have the shortest survival. The two most common diseases resulting in the need for NIV were chronic obstructive pulmonary disease (COPD) and obesity hypoventilation syndrome (OHS). The median survival time was 4.4 years in COPD subjects, but the median survival time was not reached in subjects with OHS (HR for death COPD vs. OHS: 3.2, 95% CI 1.9-5.5, <i>P</i> < 0.001). Most of the deceased subjects (55.6%) died in the hospital, while only 20.0% died at home. The last hospitalization admission leading to death occurred through the emergency room in 44.4% of the subjects.</p><p><strong>Conclusions: </strong>Survival among subjects starting NIV in this real-life study varied greatly depending on the disease and degree of functional impairment. Subjects frequently died in the hospital after admission through the emergency department. A comprehensive treatment approach with timely advance care planning is therefore needed, especially for those needing help with activities of daily living and those with both NIV and LTOT.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"8 1","pages":"1840494"},"PeriodicalIF":1.8000,"publicationDate":"2020-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/20018525.2020.1840494","citationCount":"2","resultStr":"{\"title\":\"Survival and end-of-life aspects among subjects on long-term noninvasive ventilation.\",\"authors\":\"Heidi A Rantala, Sirpa Leivo-Korpela, Siiri Kettunen, Juho T Lehto, Lauri Lehtimäki\",\"doi\":\"10.1080/20018525.2020.1840494\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The need for noninvasive ventilation (NIV) is commonly considered a predictor of poor survival, but life expectancy may vary depending on the underlying disease. We studied the factors associated with decreased survival and end-of-life characteristics in an unselected population of subjects starting NIV.</p><p><strong>Methods: </strong>We conducted a retrospective study including 205 subjects initiating NIV from 1/1/2012-31/12/2015 who were followed up until 31/12/2017.</p><p><strong>Results: </strong>The median survival time was shorter in subjects needing help with activities of daily living than in independent subjects (hazard ratio (HR) for death 1.7, 95% CI 1.2-2.6, <i>P</i> = 0.008) and was also shorter in subjects on long-term oxygen therapy (LTOT) than in those not on LTOT (HR for death 2.8, 95% CI 1.9-4.3, <i>P</i> < 0.001). There was marked difference in survival according to the disease necessitating NIV, and subjects with amyotrophic lateral sclerosis or interstitial lung disease seemed to have the shortest survival. The two most common diseases resulting in the need for NIV were chronic obstructive pulmonary disease (COPD) and obesity hypoventilation syndrome (OHS). The median survival time was 4.4 years in COPD subjects, but the median survival time was not reached in subjects with OHS (HR for death COPD vs. OHS: 3.2, 95% CI 1.9-5.5, <i>P</i> < 0.001). Most of the deceased subjects (55.6%) died in the hospital, while only 20.0% died at home. The last hospitalization admission leading to death occurred through the emergency room in 44.4% of the subjects.</p><p><strong>Conclusions: </strong>Survival among subjects starting NIV in this real-life study varied greatly depending on the disease and degree of functional impairment. Subjects frequently died in the hospital after admission through the emergency department. A comprehensive treatment approach with timely advance care planning is therefore needed, especially for those needing help with activities of daily living and those with both NIV and LTOT.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"8 1\",\"pages\":\"1840494\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1080/20018525.2020.1840494\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2020.1840494\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2020.1840494","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Survival and end-of-life aspects among subjects on long-term noninvasive ventilation.
Background: The need for noninvasive ventilation (NIV) is commonly considered a predictor of poor survival, but life expectancy may vary depending on the underlying disease. We studied the factors associated with decreased survival and end-of-life characteristics in an unselected population of subjects starting NIV.
Methods: We conducted a retrospective study including 205 subjects initiating NIV from 1/1/2012-31/12/2015 who were followed up until 31/12/2017.
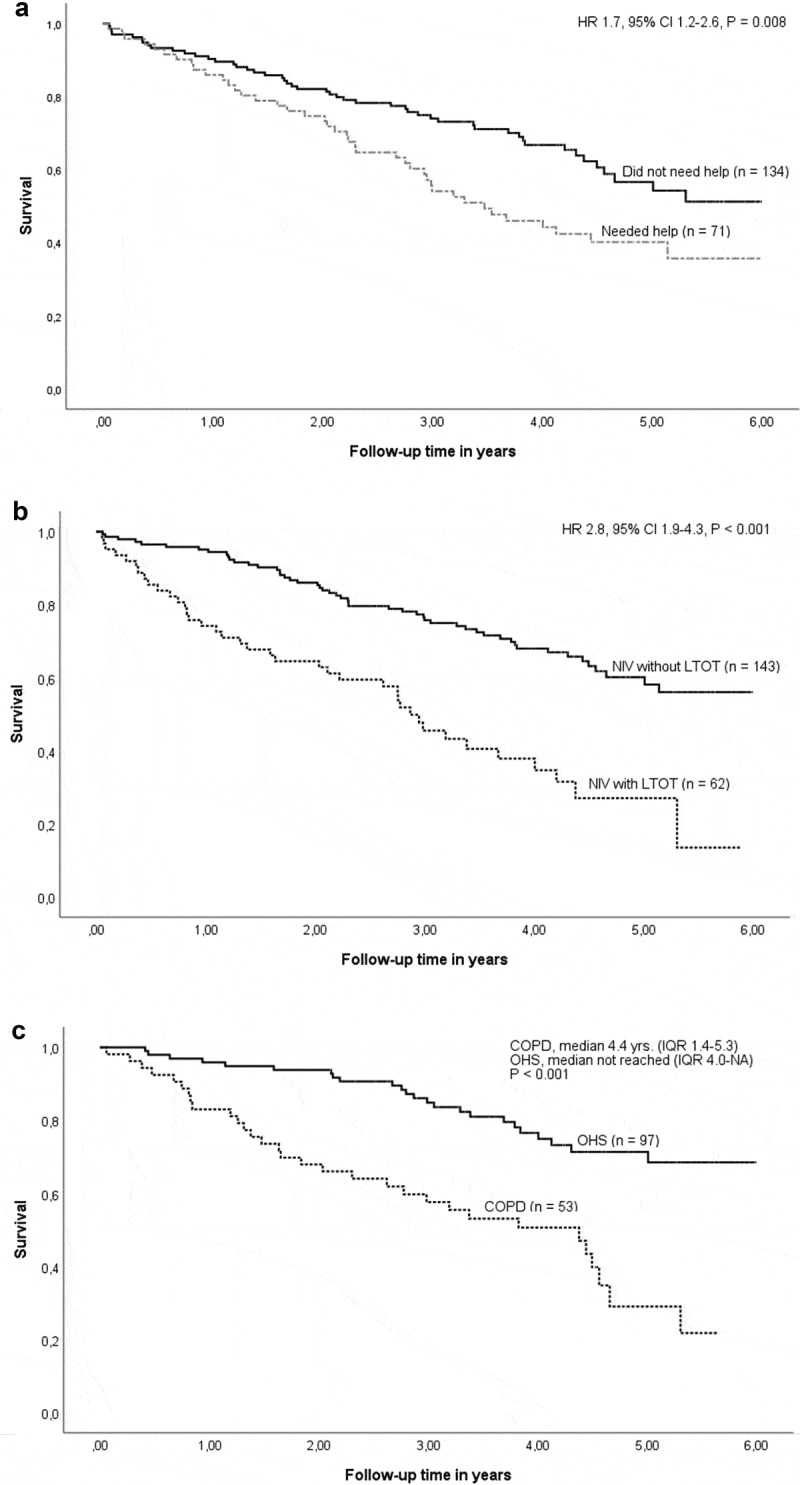
Results: The median survival time was shorter in subjects needing help with activities of daily living than in independent subjects (hazard ratio (HR) for death 1.7, 95% CI 1.2-2.6, P = 0.008) and was also shorter in subjects on long-term oxygen therapy (LTOT) than in those not on LTOT (HR for death 2.8, 95% CI 1.9-4.3, P < 0.001). There was marked difference in survival according to the disease necessitating NIV, and subjects with amyotrophic lateral sclerosis or interstitial lung disease seemed to have the shortest survival. The two most common diseases resulting in the need for NIV were chronic obstructive pulmonary disease (COPD) and obesity hypoventilation syndrome (OHS). The median survival time was 4.4 years in COPD subjects, but the median survival time was not reached in subjects with OHS (HR for death COPD vs. OHS: 3.2, 95% CI 1.9-5.5, P < 0.001). Most of the deceased subjects (55.6%) died in the hospital, while only 20.0% died at home. The last hospitalization admission leading to death occurred through the emergency room in 44.4% of the subjects.
Conclusions: Survival among subjects starting NIV in this real-life study varied greatly depending on the disease and degree of functional impairment. Subjects frequently died in the hospital after admission through the emergency department. A comprehensive treatment approach with timely advance care planning is therefore needed, especially for those needing help with activities of daily living and those with both NIV and LTOT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


