Robert Novotny, Tomas Marada, Jiri Novotny, Jakub Kristek, Jaroslav Chlupac, Michal Kudla, Kvetoslav Lipar, Jiri Mendl, Jiri Fronek, Libor Janousek
{"title":"混合修复联合新鲜同种异体动脉解剖外重建:主动脉股动脉搭桥上方并发左腹股沟感染假性动脉瘤的治疗。","authors":"Robert Novotny, Tomas Marada, Jiri Novotny, Jakub Kristek, Jaroslav Chlupac, Michal Kudla, Kvetoslav Lipar, Jiri Mendl, Jiri Fronek, Libor Janousek","doi":"10.1155/2020/8819305","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>A 72-year-old male patient was admitted into our centre with large infected pseudoaneurysm (PSA) in the left groin. The patient underwent a CT angiography (CTA) that confirmed a large partly thrombosed 6.5 × 5.5 cm PSA in the left groin arising from the distal anastomosis of the aortobifemoral bypass (ABF). Furthermore, the CTA revealed 11 cm juxtarenal abdominal aortic aneurysm (JAAA) from which the proximal anastomosis of the ABF was arising.</p><p><strong>Method: </strong>Aorto-uni-iliac stent graft Cook was placed from the right groin trough native severely stenotic right iliac arteries with proximal landing zone below the renal arteries, excluding the JAAA and the ABF. The distal landing zone was in the common iliac artery maintaining patent right internal iliac artery. Afterwards, a femoro-femoral crossover bypass from right to left was performed using a fresh arterial allograft. Postprocedurally, the hospital stay was uneventful. The left groin PSA cultures came positive for S<i>taphylococcus epidermidis</i> and <i>Corynebacterium tuberculostearicum</i>, both sensitive to vancomycin and rifampicin.</p><p><strong>Result: </strong>The patient underwent intravenous ATB treatment with vancomycin for two weeks, followed by four weeks of oral rifampicin. The patient was discharged on the 20<sup>th</sup> postoperative days.</p><p><strong>Conclusion: </strong>Hybrid repair combining aortic stent graft and extra-anatomical bypass in the treatment of infected distal parts of an aortofemoral bypass is an acceptable treatment modality.</p>","PeriodicalId":9632,"journal":{"name":"Case Reports in Vascular Medicine","volume":"2020 ","pages":"8819305"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/8819305","citationCount":"0","resultStr":"{\"title\":\"Hybrid Repair Combined with Fresh Arterial Allograft Extra-Anatomical Reconstruction: The Treatment of Infrarenal Abdominal Aneurysm above an Aortobifemoral Bypass Complicated by an Infected Pseudoaneurysm in the Left Groin.\",\"authors\":\"Robert Novotny, Tomas Marada, Jiri Novotny, Jakub Kristek, Jaroslav Chlupac, Michal Kudla, Kvetoslav Lipar, Jiri Mendl, Jiri Fronek, Libor Janousek\",\"doi\":\"10.1155/2020/8819305\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>A 72-year-old male patient was admitted into our centre with large infected pseudoaneurysm (PSA) in the left groin. The patient underwent a CT angiography (CTA) that confirmed a large partly thrombosed 6.5 × 5.5 cm PSA in the left groin arising from the distal anastomosis of the aortobifemoral bypass (ABF). Furthermore, the CTA revealed 11 cm juxtarenal abdominal aortic aneurysm (JAAA) from which the proximal anastomosis of the ABF was arising.</p><p><strong>Method: </strong>Aorto-uni-iliac stent graft Cook was placed from the right groin trough native severely stenotic right iliac arteries with proximal landing zone below the renal arteries, excluding the JAAA and the ABF. The distal landing zone was in the common iliac artery maintaining patent right internal iliac artery. Afterwards, a femoro-femoral crossover bypass from right to left was performed using a fresh arterial allograft. Postprocedurally, the hospital stay was uneventful. The left groin PSA cultures came positive for S<i>taphylococcus epidermidis</i> and <i>Corynebacterium tuberculostearicum</i>, both sensitive to vancomycin and rifampicin.</p><p><strong>Result: </strong>The patient underwent intravenous ATB treatment with vancomycin for two weeks, followed by four weeks of oral rifampicin. The patient was discharged on the 20<sup>th</sup> postoperative days.</p><p><strong>Conclusion: </strong>Hybrid repair combining aortic stent graft and extra-anatomical bypass in the treatment of infected distal parts of an aortofemoral bypass is an acceptable treatment modality.</p>\",\"PeriodicalId\":9632,\"journal\":{\"name\":\"Case Reports in Vascular Medicine\",\"volume\":\"2020 \",\"pages\":\"8819305\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/8819305\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Vascular Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/8819305\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Vascular Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/8819305","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Hybrid Repair Combined with Fresh Arterial Allograft Extra-Anatomical Reconstruction: The Treatment of Infrarenal Abdominal Aneurysm above an Aortobifemoral Bypass Complicated by an Infected Pseudoaneurysm in the Left Groin.
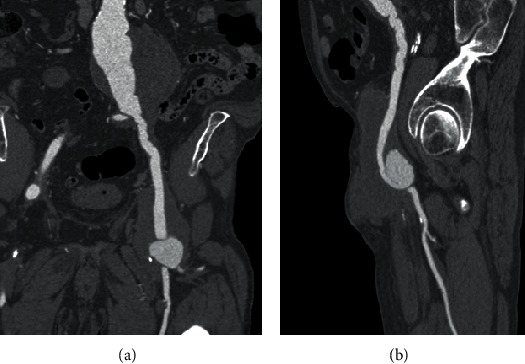
Introduction: A 72-year-old male patient was admitted into our centre with large infected pseudoaneurysm (PSA) in the left groin. The patient underwent a CT angiography (CTA) that confirmed a large partly thrombosed 6.5 × 5.5 cm PSA in the left groin arising from the distal anastomosis of the aortobifemoral bypass (ABF). Furthermore, the CTA revealed 11 cm juxtarenal abdominal aortic aneurysm (JAAA) from which the proximal anastomosis of the ABF was arising.
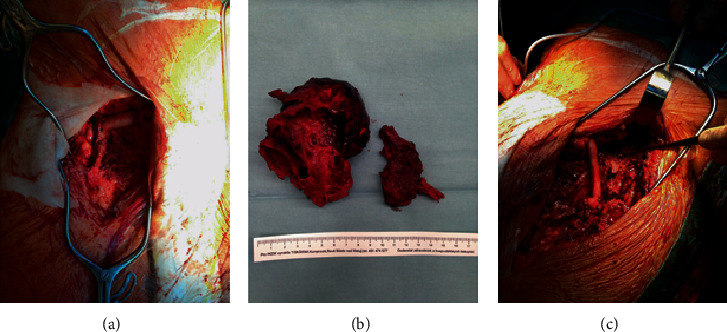
Method: Aorto-uni-iliac stent graft Cook was placed from the right groin trough native severely stenotic right iliac arteries with proximal landing zone below the renal arteries, excluding the JAAA and the ABF. The distal landing zone was in the common iliac artery maintaining patent right internal iliac artery. Afterwards, a femoro-femoral crossover bypass from right to left was performed using a fresh arterial allograft. Postprocedurally, the hospital stay was uneventful. The left groin PSA cultures came positive for Staphylococcus epidermidis and Corynebacterium tuberculostearicum, both sensitive to vancomycin and rifampicin.
Result: The patient underwent intravenous ATB treatment with vancomycin for two weeks, followed by four weeks of oral rifampicin. The patient was discharged on the 20th postoperative days.
Conclusion: Hybrid repair combining aortic stent graft and extra-anatomical bypass in the treatment of infected distal parts of an aortofemoral bypass is an acceptable treatment modality.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


