{"title":"COVID-19与肺血管损伤","authors":"Hai-Long Dai, Xue-Feng Guang","doi":"10.1177/1470320320972276","DOIUrl":null,"url":null,"abstract":"Creative Commons Non Commercial CC BY-NC: This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 License (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages (https://us.sagepub.com/en-us/nam/open-access-at-sage). Dear Sir, Since December 2019, an outbreak of coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in Wuhan, which imposes significant threats to global public health. Studies found that SARS-CoV-2 and SARS-Cov share the same receptor, angiotensin-converting enzyme 2 (ACE2),1,2 SARS-CoV-2 have a 10to 20-fold higher affinity for ACE2 than SARS-CoV,3 and the pathogenic mechanism may be shared between these two viruses.4 The renin–angiotensin system (RAS) plays important role in cardiovascular system. ACE2, a homolog of ACE, is a carboxypeptidase that degrades angiotensin (Ang) II to Ang-(1–7). ACE2 plays an important role in the vasodilative axis (ACE2–Ang-(1–7)–Mas axis) of the RAS and counterbalances the vasoconstrictive, proliferative, and fibrotic axes (ACE–Ang II–Ang II type 1 receptor (AT1R) axis) of the RAS.5 ACE2 is highly expressed in the lungs and heart. Since then, an abundance of evidence has supported the fundamental concept that ACE2 is protective against a variety of cardiopulmonary vascular diseases, including heart failure, hypertension, pulmonary arterial hypertension (PAH).6–8 In the lungs, activation of local pulmonary RAS can affect the pathogenesis of lung injury, high levels of Ang II can lead to increases in vascular permeability and alterations of alveolar epithelial cells.9 In SARS-CoV infection of mice, both viral replication and the viral spike protein alone have been shown to selectively reduce ACE2.10 SARS-CoV also induces rapid downregulation of ACE2 from the cell surface.11 The entry of SARS-CoV2 into the cells through membrane fusion also markedly down-regulates ACE2 receptors.12 Balancing ACE/ACE2 axis may be alleviate virus-induced severe lung injury. ACE Inhibitors (ACEIs) and Angiotensin Receptor Blockers (ARBs) may help reduce lung injury caused by viral infection.13,14 So, for SARS-CoV-2 infected patients with hypertension, ACEIs and ARBs may be a good choice.15–17 ACE2 is also expressed in endothelial cells, especially lung microvascular endothelial cell.18–20 The decrease of ACE2 is related to pulmonary vascular remodeling and PAH.21 These results suggest that SARS-CoV-2 infection may cause pulmonary vascular injury and remodeling by disrupted the balance between ACE/ACE2 and Ang II/ Ang-(1–7) (Figure 1). ACE2 has been shown to be decreased in the plasma of patients with PAH, those patients are more likely to develop into severe patients after SARS-CoV-2 infection. So, we suggest that special care of pulmonary vascular injury should be installed in treating SARS-CoV-2 patients during the hospitalization, and clinical follow up of lung function and pulmonary arterial pressure after cure. COVID-19 and the pulmonary vascular injury","PeriodicalId":17330,"journal":{"name":"Journal of the Renin-Angiotensin-Aldosterone System","volume":"21 4","pages":"1470320320972276"},"PeriodicalIF":4.1000,"publicationDate":"2020-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1470320320972276","citationCount":"0","resultStr":"{\"title\":\"COVID-19 and the pulmonary vascular injury.\",\"authors\":\"Hai-Long Dai, Xue-Feng Guang\",\"doi\":\"10.1177/1470320320972276\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Creative Commons Non Commercial CC BY-NC: This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 License (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages (https://us.sagepub.com/en-us/nam/open-access-at-sage). Dear Sir, Since December 2019, an outbreak of coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in Wuhan, which imposes significant threats to global public health. Studies found that SARS-CoV-2 and SARS-Cov share the same receptor, angiotensin-converting enzyme 2 (ACE2),1,2 SARS-CoV-2 have a 10to 20-fold higher affinity for ACE2 than SARS-CoV,3 and the pathogenic mechanism may be shared between these two viruses.4 The renin–angiotensin system (RAS) plays important role in cardiovascular system. ACE2, a homolog of ACE, is a carboxypeptidase that degrades angiotensin (Ang) II to Ang-(1–7). ACE2 plays an important role in the vasodilative axis (ACE2–Ang-(1–7)–Mas axis) of the RAS and counterbalances the vasoconstrictive, proliferative, and fibrotic axes (ACE–Ang II–Ang II type 1 receptor (AT1R) axis) of the RAS.5 ACE2 is highly expressed in the lungs and heart. Since then, an abundance of evidence has supported the fundamental concept that ACE2 is protective against a variety of cardiopulmonary vascular diseases, including heart failure, hypertension, pulmonary arterial hypertension (PAH).6–8 In the lungs, activation of local pulmonary RAS can affect the pathogenesis of lung injury, high levels of Ang II can lead to increases in vascular permeability and alterations of alveolar epithelial cells.9 In SARS-CoV infection of mice, both viral replication and the viral spike protein alone have been shown to selectively reduce ACE2.10 SARS-CoV also induces rapid downregulation of ACE2 from the cell surface.11 The entry of SARS-CoV2 into the cells through membrane fusion also markedly down-regulates ACE2 receptors.12 Balancing ACE/ACE2 axis may be alleviate virus-induced severe lung injury. ACE Inhibitors (ACEIs) and Angiotensin Receptor Blockers (ARBs) may help reduce lung injury caused by viral infection.13,14 So, for SARS-CoV-2 infected patients with hypertension, ACEIs and ARBs may be a good choice.15–17 ACE2 is also expressed in endothelial cells, especially lung microvascular endothelial cell.18–20 The decrease of ACE2 is related to pulmonary vascular remodeling and PAH.21 These results suggest that SARS-CoV-2 infection may cause pulmonary vascular injury and remodeling by disrupted the balance between ACE/ACE2 and Ang II/ Ang-(1–7) (Figure 1). ACE2 has been shown to be decreased in the plasma of patients with PAH, those patients are more likely to develop into severe patients after SARS-CoV-2 infection. So, we suggest that special care of pulmonary vascular injury should be installed in treating SARS-CoV-2 patients during the hospitalization, and clinical follow up of lung function and pulmonary arterial pressure after cure. COVID-19 and the pulmonary vascular injury\",\"PeriodicalId\":17330,\"journal\":{\"name\":\"Journal of the Renin-Angiotensin-Aldosterone System\",\"volume\":\"21 4\",\"pages\":\"1470320320972276\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2020-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1470320320972276\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Renin-Angiotensin-Aldosterone System\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/1470320320972276\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Renin-Angiotensin-Aldosterone System","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/1470320320972276","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
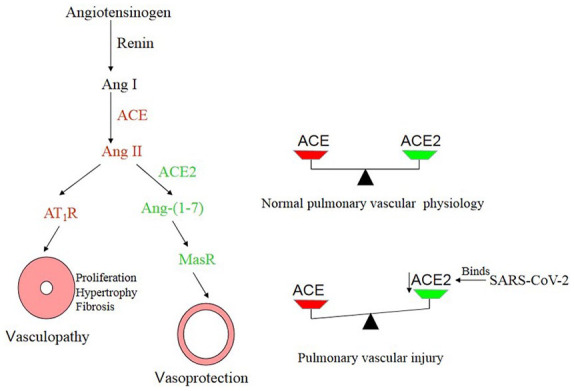
Creative Commons Non Commercial CC BY-NC: This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 License (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages (https://us.sagepub.com/en-us/nam/open-access-at-sage). Dear Sir, Since December 2019, an outbreak of coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in Wuhan, which imposes significant threats to global public health. Studies found that SARS-CoV-2 and SARS-Cov share the same receptor, angiotensin-converting enzyme 2 (ACE2),1,2 SARS-CoV-2 have a 10to 20-fold higher affinity for ACE2 than SARS-CoV,3 and the pathogenic mechanism may be shared between these two viruses.4 The renin–angiotensin system (RAS) plays important role in cardiovascular system. ACE2, a homolog of ACE, is a carboxypeptidase that degrades angiotensin (Ang) II to Ang-(1–7). ACE2 plays an important role in the vasodilative axis (ACE2–Ang-(1–7)–Mas axis) of the RAS and counterbalances the vasoconstrictive, proliferative, and fibrotic axes (ACE–Ang II–Ang II type 1 receptor (AT1R) axis) of the RAS.5 ACE2 is highly expressed in the lungs and heart. Since then, an abundance of evidence has supported the fundamental concept that ACE2 is protective against a variety of cardiopulmonary vascular diseases, including heart failure, hypertension, pulmonary arterial hypertension (PAH).6–8 In the lungs, activation of local pulmonary RAS can affect the pathogenesis of lung injury, high levels of Ang II can lead to increases in vascular permeability and alterations of alveolar epithelial cells.9 In SARS-CoV infection of mice, both viral replication and the viral spike protein alone have been shown to selectively reduce ACE2.10 SARS-CoV also induces rapid downregulation of ACE2 from the cell surface.11 The entry of SARS-CoV2 into the cells through membrane fusion also markedly down-regulates ACE2 receptors.12 Balancing ACE/ACE2 axis may be alleviate virus-induced severe lung injury. ACE Inhibitors (ACEIs) and Angiotensin Receptor Blockers (ARBs) may help reduce lung injury caused by viral infection.13,14 So, for SARS-CoV-2 infected patients with hypertension, ACEIs and ARBs may be a good choice.15–17 ACE2 is also expressed in endothelial cells, especially lung microvascular endothelial cell.18–20 The decrease of ACE2 is related to pulmonary vascular remodeling and PAH.21 These results suggest that SARS-CoV-2 infection may cause pulmonary vascular injury and remodeling by disrupted the balance between ACE/ACE2 and Ang II/ Ang-(1–7) (Figure 1). ACE2 has been shown to be decreased in the plasma of patients with PAH, those patients are more likely to develop into severe patients after SARS-CoV-2 infection. So, we suggest that special care of pulmonary vascular injury should be installed in treating SARS-CoV-2 patients during the hospitalization, and clinical follow up of lung function and pulmonary arterial pressure after cure. COVID-19 and the pulmonary vascular injury
期刊介绍:
JRAAS is a peer-reviewed, open access journal, serving as a resource for biomedical professionals, primarily with an active interest in the renin-angiotensin-aldosterone system in humans and other mammals. It publishes original research and reviews on the normal and abnormal function of this system and its pharmacology and therapeutics, mostly in a cardiovascular context but including research in all areas where this system is present, including the brain, lungs and gastro-intestinal tract.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


