Monija Mrgan, Bjarne Linde Nørgaard, Damini Dey, Jørgen Gram, Michael Hecht Olsen, Jeppe Gram, Niels Peter Rønnow Sand
{"title":"早期 2 型糖尿病无症状患者的冠状动脉血流损伤:通过 FFRCT 检测。","authors":"Monija Mrgan, Bjarne Linde Nørgaard, Damini Dey, Jørgen Gram, Michael Hecht Olsen, Jeppe Gram, Niels Peter Rønnow Sand","doi":"10.1177/1479164120958422","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To determine the occurrence of physiological significant coronary artery disease (CAD) by coronary CT angiography (CTA) derived fractional flow reserve (FFR<sub>CT</sub>) in asymptomatic patients with a new diagnosis (<1 year) of type-2 diabetes mellitus (T2DM).</p><p><strong>Methods: </strong>FFR<sub>CT</sub>-analysis was performed from standard acquired coronary CTA data sets. The per-patient minimum distal FFR<sub>CT</sub>-value (d-FFR<sub>CT</sub>) in coronary vessels (diameter ⩾1.8 mm) was registered. The threshold for categorizing FFR<sub>CT</sub>-analysis as abnormal was a d-FFR<sub>CT</sub> ⩽0.75. Total plaque volume and volumes of calcified plaque, non-calcified plaque, and low-density non-calcified plaque (LD-NCP) were assessed by quantitative plaque analysis.</p><p><strong>Results: </strong>Overall, 76 patients; age, mean (SD): 56 (11) years; males, <i>n</i> (%): 49(65), were studied. A total of 57% of patients had plaques. The d-FFR<sub>CT</sub> was ⩽0.75 in 12 (16%) patients. The d-FFR<sub>CT</sub>, median (IQR), was 0.84 (0.79-0.87). Median (range) d-FFR<sub>CT</sub> in patients with d-FFR<sub>CT</sub> ⩽0.75 was 0.70 (0.6-0.74). Patients with d-FFR<sub>CT</sub>⩽0.75 versus d-FFR<sub>CT</sub> >0.75 had numerically higher plaque volumes for all plaques components, although only significant for the LD-NCP component.</p><p><strong>Conclusion: </strong>Every sixth asymptomatic patient with a new diagnosis of T2DM has hemodynamic significant CAD as evaluated by FFR<sub>CT.</sub> Flow impairment by FFR<sub>CT</sub> was associated with coronary plaque characteristics.</p>","PeriodicalId":11092,"journal":{"name":"Diabetes & Vascular Disease Research","volume":"17 9","pages":"1479164120958422"},"PeriodicalIF":2.8000,"publicationDate":"2020-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/cf/10.1177_1479164120958422.PMC7919222.pdf","citationCount":"0","resultStr":"{\"title\":\"Coronary flow impairment in asymptomatic patients with early stage type-2 diabetes: Detection by FFR<sub>CT</sub>.\",\"authors\":\"Monija Mrgan, Bjarne Linde Nørgaard, Damini Dey, Jørgen Gram, Michael Hecht Olsen, Jeppe Gram, Niels Peter Rønnow Sand\",\"doi\":\"10.1177/1479164120958422\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To determine the occurrence of physiological significant coronary artery disease (CAD) by coronary CT angiography (CTA) derived fractional flow reserve (FFR<sub>CT</sub>) in asymptomatic patients with a new diagnosis (<1 year) of type-2 diabetes mellitus (T2DM).</p><p><strong>Methods: </strong>FFR<sub>CT</sub>-analysis was performed from standard acquired coronary CTA data sets. The per-patient minimum distal FFR<sub>CT</sub>-value (d-FFR<sub>CT</sub>) in coronary vessels (diameter ⩾1.8 mm) was registered. The threshold for categorizing FFR<sub>CT</sub>-analysis as abnormal was a d-FFR<sub>CT</sub> ⩽0.75. Total plaque volume and volumes of calcified plaque, non-calcified plaque, and low-density non-calcified plaque (LD-NCP) were assessed by quantitative plaque analysis.</p><p><strong>Results: </strong>Overall, 76 patients; age, mean (SD): 56 (11) years; males, <i>n</i> (%): 49(65), were studied. A total of 57% of patients had plaques. The d-FFR<sub>CT</sub> was ⩽0.75 in 12 (16%) patients. The d-FFR<sub>CT</sub>, median (IQR), was 0.84 (0.79-0.87). Median (range) d-FFR<sub>CT</sub> in patients with d-FFR<sub>CT</sub> ⩽0.75 was 0.70 (0.6-0.74). Patients with d-FFR<sub>CT</sub>⩽0.75 versus d-FFR<sub>CT</sub> >0.75 had numerically higher plaque volumes for all plaques components, although only significant for the LD-NCP component.</p><p><strong>Conclusion: </strong>Every sixth asymptomatic patient with a new diagnosis of T2DM has hemodynamic significant CAD as evaluated by FFR<sub>CT.</sub> Flow impairment by FFR<sub>CT</sub> was associated with coronary plaque characteristics.</p>\",\"PeriodicalId\":11092,\"journal\":{\"name\":\"Diabetes & Vascular Disease Research\",\"volume\":\"17 9\",\"pages\":\"1479164120958422\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2020-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/cf/10.1177_1479164120958422.PMC7919222.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes & Vascular Disease Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/1479164120958422\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes & Vascular Disease Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/1479164120958422","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Coronary flow impairment in asymptomatic patients with early stage type-2 diabetes: Detection by FFRCT.
Purpose: To determine the occurrence of physiological significant coronary artery disease (CAD) by coronary CT angiography (CTA) derived fractional flow reserve (FFRCT) in asymptomatic patients with a new diagnosis (<1 year) of type-2 diabetes mellitus (T2DM).
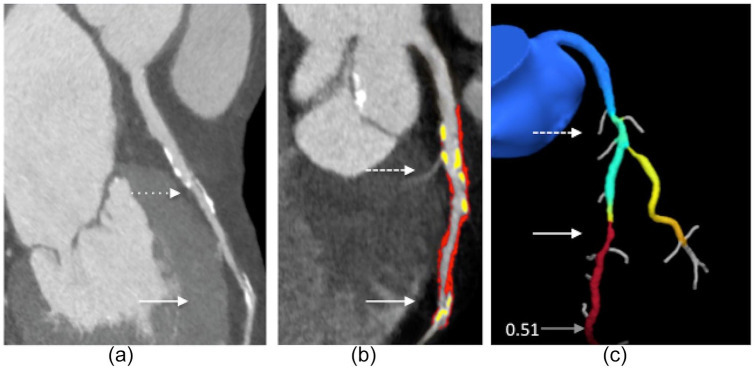
Methods: FFRCT-analysis was performed from standard acquired coronary CTA data sets. The per-patient minimum distal FFRCT-value (d-FFRCT) in coronary vessels (diameter ⩾1.8 mm) was registered. The threshold for categorizing FFRCT-analysis as abnormal was a d-FFRCT ⩽0.75. Total plaque volume and volumes of calcified plaque, non-calcified plaque, and low-density non-calcified plaque (LD-NCP) were assessed by quantitative plaque analysis.
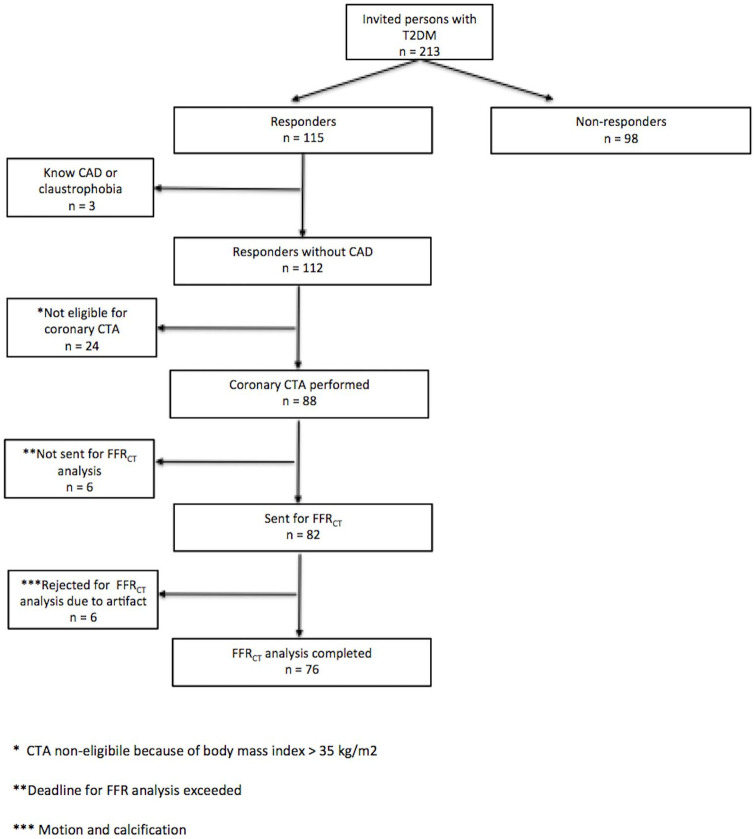
Results: Overall, 76 patients; age, mean (SD): 56 (11) years; males, n (%): 49(65), were studied. A total of 57% of patients had plaques. The d-FFRCT was ⩽0.75 in 12 (16%) patients. The d-FFRCT, median (IQR), was 0.84 (0.79-0.87). Median (range) d-FFRCT in patients with d-FFRCT ⩽0.75 was 0.70 (0.6-0.74). Patients with d-FFRCT⩽0.75 versus d-FFRCT >0.75 had numerically higher plaque volumes for all plaques components, although only significant for the LD-NCP component.
Conclusion: Every sixth asymptomatic patient with a new diagnosis of T2DM has hemodynamic significant CAD as evaluated by FFRCT. Flow impairment by FFRCT was associated with coronary plaque characteristics.
期刊介绍:
Diabetes & Vascular Disease Research is the first international peer-reviewed journal to unite diabetes and vascular disease in a single title. The journal publishes original papers, research letters and reviews. This journal is a member of the Committee on Publication Ethics (COPE)


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


