Aysun Ata, Samim Özen, Damla Gökşen, Neslihan Edeer Karaca, Güzide Aksu, Necil Kütükçüler, Hüseyin Onay, Şükran Darcan
{"title":"1例11岁男童全身性毛细血管渗漏综合征与糖尿病显著共存:1例报告及文献复习。","authors":"Aysun Ata, Samim Özen, Damla Gökşen, Neslihan Edeer Karaca, Güzide Aksu, Necil Kütükçüler, Hüseyin Onay, Şükran Darcan","doi":"10.1155/2020/8891902","DOIUrl":null,"url":null,"abstract":"<p><p>Systemic capillary leak syndrome (ISCLS) is a rare disease characterized by unexplained reversible capillary hyperpermeability followed by hypoperfusion, hemoconcentration, and either hypoalbuminemia or total hypoproteinemia. An 11-year-old boy was admitted with vomiting, generalized edema, and hyperglycemia, which was preceded by 5 days of coryzal symptoms, lethargy, and oral aft, without fever. On physical examination, he had tachycardia and hypotension, with severe generalized systemic nonitchy edema, and the laboratory tests supported the conclusion that he had severe hemoconcentration with hemoglobin: 184 g/L, hematocrit: 51.3 %, urea: 20 mmol/L, blood glucose: 11.1 mmol/L, and albumin: 19 gr/L, with normal urine analysis. On the fourth day, the patient was diagnosed with ISCLS, by ruling out other causes of shock and hypoalbuminemia. Intravenous immunoglobulin (IVIG) treatment regimen was administered on two consecutive days (day five and day six). His edema decreased on the fifth day, and the patient was deemed clinically well. There was no compartment syndrome, rhabdomyolysis, or pulmonary edema in the recovery period. However, respiratory virus panel PCR was positive for respiratory syncytial virus (RSV) and enterovirus, which were thought to be the triggering cause of ISCLS. For the differential diagnosis of diabetes, his fasting serum glucose was 13.4 mmol/L, simultaneous C-peptide was 0.44 nmol/L, and HbA1c was 64 mmol/mol, and urine ketone was positive. However, antiglutamic acid decarboxylase, anti-insulin antibody, and islet cell antibody were negative. At the last outpatient visit, 22 months after the diagnosis, his insulin dose was still 0.4 IU/kg/day and HbA1c was 40 mmol/mol, and without prophylaxis, there was no ISCLS attack. <i>Conclusion</i>. Early recognition of ISCLS is important for therapeutic awareness, since it is very rare in childhood and occurs usually without any prior provoking factors in healthy children. With the increase in awareness of the disease, knowledge and experiences about pediatric patients may also increase. We think that our case will contribute to the literature since there have been no pediatric diabetic patients with ISCLS reported.</p>","PeriodicalId":42865,"journal":{"name":"Case Reports in Immunology","volume":"2020 ","pages":"8891902"},"PeriodicalIF":1.5000,"publicationDate":"2020-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/8891902","citationCount":"0","resultStr":"{\"title\":\"A Remarkable Coexistence of Systemic Capillary Leak Syndrome and Diabetes in an 11-Year-Old Boy: A Case Report and Review of the Literature.\",\"authors\":\"Aysun Ata, Samim Özen, Damla Gökşen, Neslihan Edeer Karaca, Güzide Aksu, Necil Kütükçüler, Hüseyin Onay, Şükran Darcan\",\"doi\":\"10.1155/2020/8891902\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Systemic capillary leak syndrome (ISCLS) is a rare disease characterized by unexplained reversible capillary hyperpermeability followed by hypoperfusion, hemoconcentration, and either hypoalbuminemia or total hypoproteinemia. An 11-year-old boy was admitted with vomiting, generalized edema, and hyperglycemia, which was preceded by 5 days of coryzal symptoms, lethargy, and oral aft, without fever. On physical examination, he had tachycardia and hypotension, with severe generalized systemic nonitchy edema, and the laboratory tests supported the conclusion that he had severe hemoconcentration with hemoglobin: 184 g/L, hematocrit: 51.3 %, urea: 20 mmol/L, blood glucose: 11.1 mmol/L, and albumin: 19 gr/L, with normal urine analysis. On the fourth day, the patient was diagnosed with ISCLS, by ruling out other causes of shock and hypoalbuminemia. Intravenous immunoglobulin (IVIG) treatment regimen was administered on two consecutive days (day five and day six). His edema decreased on the fifth day, and the patient was deemed clinically well. There was no compartment syndrome, rhabdomyolysis, or pulmonary edema in the recovery period. However, respiratory virus panel PCR was positive for respiratory syncytial virus (RSV) and enterovirus, which were thought to be the triggering cause of ISCLS. For the differential diagnosis of diabetes, his fasting serum glucose was 13.4 mmol/L, simultaneous C-peptide was 0.44 nmol/L, and HbA1c was 64 mmol/mol, and urine ketone was positive. However, antiglutamic acid decarboxylase, anti-insulin antibody, and islet cell antibody were negative. At the last outpatient visit, 22 months after the diagnosis, his insulin dose was still 0.4 IU/kg/day and HbA1c was 40 mmol/mol, and without prophylaxis, there was no ISCLS attack. <i>Conclusion</i>. Early recognition of ISCLS is important for therapeutic awareness, since it is very rare in childhood and occurs usually without any prior provoking factors in healthy children. With the increase in awareness of the disease, knowledge and experiences about pediatric patients may also increase. We think that our case will contribute to the literature since there have been no pediatric diabetic patients with ISCLS reported.</p>\",\"PeriodicalId\":42865,\"journal\":{\"name\":\"Case Reports in Immunology\",\"volume\":\"2020 \",\"pages\":\"8891902\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2020-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/8891902\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Immunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/8891902\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/8891902","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
A Remarkable Coexistence of Systemic Capillary Leak Syndrome and Diabetes in an 11-Year-Old Boy: A Case Report and Review of the Literature.
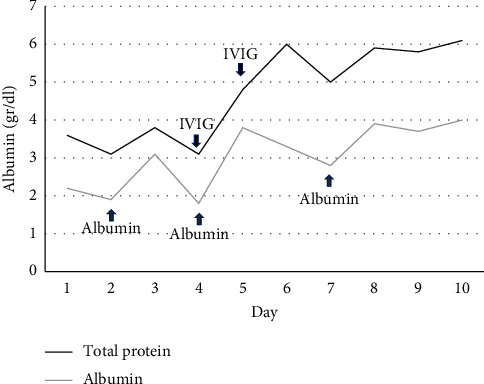
Systemic capillary leak syndrome (ISCLS) is a rare disease characterized by unexplained reversible capillary hyperpermeability followed by hypoperfusion, hemoconcentration, and either hypoalbuminemia or total hypoproteinemia. An 11-year-old boy was admitted with vomiting, generalized edema, and hyperglycemia, which was preceded by 5 days of coryzal symptoms, lethargy, and oral aft, without fever. On physical examination, he had tachycardia and hypotension, with severe generalized systemic nonitchy edema, and the laboratory tests supported the conclusion that he had severe hemoconcentration with hemoglobin: 184 g/L, hematocrit: 51.3 %, urea: 20 mmol/L, blood glucose: 11.1 mmol/L, and albumin: 19 gr/L, with normal urine analysis. On the fourth day, the patient was diagnosed with ISCLS, by ruling out other causes of shock and hypoalbuminemia. Intravenous immunoglobulin (IVIG) treatment regimen was administered on two consecutive days (day five and day six). His edema decreased on the fifth day, and the patient was deemed clinically well. There was no compartment syndrome, rhabdomyolysis, or pulmonary edema in the recovery period. However, respiratory virus panel PCR was positive for respiratory syncytial virus (RSV) and enterovirus, which were thought to be the triggering cause of ISCLS. For the differential diagnosis of diabetes, his fasting serum glucose was 13.4 mmol/L, simultaneous C-peptide was 0.44 nmol/L, and HbA1c was 64 mmol/mol, and urine ketone was positive. However, antiglutamic acid decarboxylase, anti-insulin antibody, and islet cell antibody were negative. At the last outpatient visit, 22 months after the diagnosis, his insulin dose was still 0.4 IU/kg/day and HbA1c was 40 mmol/mol, and without prophylaxis, there was no ISCLS attack. Conclusion. Early recognition of ISCLS is important for therapeutic awareness, since it is very rare in childhood and occurs usually without any prior provoking factors in healthy children. With the increase in awareness of the disease, knowledge and experiences about pediatric patients may also increase. We think that our case will contribute to the literature since there have been no pediatric diabetic patients with ISCLS reported.
期刊介绍:
Case Reports in Immunology is a peer-reviewed, Open Access journal that publishes case reports and case series related to allergies, immunodeficiencies, autoimmune diseases, immune disorders, cancer immunology and transplantation immunology.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


