Hong Rae Kim, Sung-Ho Jung, Junho Yang, Min Su Kim, Tae-Jin Yun, Jae-Joong Kim, Jae Won Lee
{"title":"吻合前补充停搏液输注对长缺血时间心脏移植患者的影响。","authors":"Hong Rae Kim, Sung-Ho Jung, Junho Yang, Min Su Kim, Tae-Jin Yun, Jae-Joong Kim, Jae Won Lee","doi":"10.5090/kjtcs.19.091","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prolonged ischemic time is a risk factor for primary graft dysfunction in patients who undergo heart transplantation. We investigated the effect of a supplemental cardioplegia infusion before anastomosis in patients with long ischemic times.</p><p><strong>Methods: </strong>We identified 236 consecutive patients who underwent orthotopic heart transplantation between February 2010 and December 2014. Among them, the patients with total ischemic times of longer than 3 hours (n=59) were categorized based on whether they were administered a complementary cardioplegia solution (CPS) immediately before implantation (CPS+, n=30; CPS-, n=29).</p><p><strong>Results: </strong>The mean total ischemic times in the CPS+ and CPS- groups were 238.1±30.1 minutes and 230.1±28.2 minutes, respectively (p=0.3). The incidence of left ventricular primary graft dysfunction (CPS+, n=6 [20.0%]; CPS-, n=5 [17.2%]; p=0.79) was comparable between the groups. In the Kaplan-Meier survival analysis, no significant difference in overall survival at 5 years was observed between the CPS+ and CPS- groups (83.1%±6.9% vs. 89.7%±5.7%, respectively; log-rank p=0.7). No inter-group differences in early mortality (CPS+, n=0; CPS-, n=1 [3.4%]; p=0.98) or complications were observed.</p><p><strong>Conclusion: </strong>The additional infusion of a cardioplegia solution immediately before implantation in patients with longer ischemic times is a simple, reproducible, and safe procedure. However, we did not observe benefits of this strategy in the present study.</p>","PeriodicalId":38678,"journal":{"name":"Korean Journal of Thoracic and Cardiovascular Surgery","volume":"53 6","pages":"375-380"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/6c/KJTCV-53-375.PMC7721527.pdf","citationCount":"0","resultStr":"{\"title\":\"The Effect of Supplemental Cardioplegia Infusion before Anastomosis in Patients Undergoing Heart Transplantation with Long Ischemic Times.\",\"authors\":\"Hong Rae Kim, Sung-Ho Jung, Junho Yang, Min Su Kim, Tae-Jin Yun, Jae-Joong Kim, Jae Won Lee\",\"doi\":\"10.5090/kjtcs.19.091\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prolonged ischemic time is a risk factor for primary graft dysfunction in patients who undergo heart transplantation. We investigated the effect of a supplemental cardioplegia infusion before anastomosis in patients with long ischemic times.</p><p><strong>Methods: </strong>We identified 236 consecutive patients who underwent orthotopic heart transplantation between February 2010 and December 2014. Among them, the patients with total ischemic times of longer than 3 hours (n=59) were categorized based on whether they were administered a complementary cardioplegia solution (CPS) immediately before implantation (CPS+, n=30; CPS-, n=29).</p><p><strong>Results: </strong>The mean total ischemic times in the CPS+ and CPS- groups were 238.1±30.1 minutes and 230.1±28.2 minutes, respectively (p=0.3). The incidence of left ventricular primary graft dysfunction (CPS+, n=6 [20.0%]; CPS-, n=5 [17.2%]; p=0.79) was comparable between the groups. In the Kaplan-Meier survival analysis, no significant difference in overall survival at 5 years was observed between the CPS+ and CPS- groups (83.1%±6.9% vs. 89.7%±5.7%, respectively; log-rank p=0.7). No inter-group differences in early mortality (CPS+, n=0; CPS-, n=1 [3.4%]; p=0.98) or complications were observed.</p><p><strong>Conclusion: </strong>The additional infusion of a cardioplegia solution immediately before implantation in patients with longer ischemic times is a simple, reproducible, and safe procedure. However, we did not observe benefits of this strategy in the present study.</p>\",\"PeriodicalId\":38678,\"journal\":{\"name\":\"Korean Journal of Thoracic and Cardiovascular Surgery\",\"volume\":\"53 6\",\"pages\":\"375-380\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-12-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/6c/KJTCV-53-375.PMC7721527.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5090/kjtcs.19.091\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/kjtcs.19.091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:缺血时间延长是心脏移植患者原发性移植物功能障碍的危险因素。我们研究了吻合前补充停搏液输注对缺血时间过长的患者的影响。方法:我们选取了2010年2月至2014年12月期间连续接受原位心脏移植的236例患者。其中,总缺血时间大于3小时的患者(n=59)根据是否在植入前立即给予补心停搏液(CPS+, n=30;CPS - n = 29)。结果:CPS+组和CPS-组的平均总缺血时间分别为238.1±30.1 min和230.1±28.2 min (p=0.3)。左心室原发性移植物功能障碍发生率(CPS+, n=6 [20.0%];CPS-, n=5 [17.2%];P =0.79)组间具有可比性。在Kaplan-Meier生存分析中,CPS+组和CPS-组的5年总生存率无显著差异(分别为83.1%±6.9%和89.7%±5.7%;log-rank p = 0.7)。早期死亡率组间无差异(CPS+, n=0;CPS-, n=1 [3.4%];P =0.98)或出现并发症。结论:对于缺血时间较长的患者,在植入前立即输液停搏液是一种简单、可重复且安全的方法。然而,在目前的研究中,我们没有观察到这种策略的好处。
The Effect of Supplemental Cardioplegia Infusion before Anastomosis in Patients Undergoing Heart Transplantation with Long Ischemic Times.
Background: Prolonged ischemic time is a risk factor for primary graft dysfunction in patients who undergo heart transplantation. We investigated the effect of a supplemental cardioplegia infusion before anastomosis in patients with long ischemic times.
Methods: We identified 236 consecutive patients who underwent orthotopic heart transplantation between February 2010 and December 2014. Among them, the patients with total ischemic times of longer than 3 hours (n=59) were categorized based on whether they were administered a complementary cardioplegia solution (CPS) immediately before implantation (CPS+, n=30; CPS-, n=29).
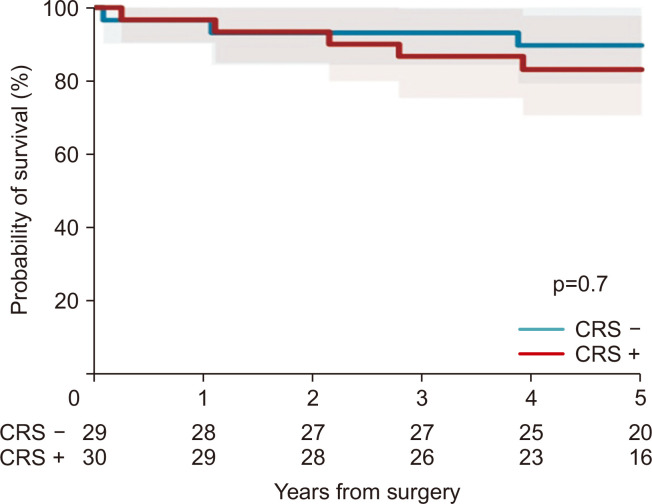
Results: The mean total ischemic times in the CPS+ and CPS- groups were 238.1±30.1 minutes and 230.1±28.2 minutes, respectively (p=0.3). The incidence of left ventricular primary graft dysfunction (CPS+, n=6 [20.0%]; CPS-, n=5 [17.2%]; p=0.79) was comparable between the groups. In the Kaplan-Meier survival analysis, no significant difference in overall survival at 5 years was observed between the CPS+ and CPS- groups (83.1%±6.9% vs. 89.7%±5.7%, respectively; log-rank p=0.7). No inter-group differences in early mortality (CPS+, n=0; CPS-, n=1 [3.4%]; p=0.98) or complications were observed.
Conclusion: The additional infusion of a cardioplegia solution immediately before implantation in patients with longer ischemic times is a simple, reproducible, and safe procedure. However, we did not observe benefits of this strategy in the present study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


