Judith Bellapart, Vinesh Appadurai, Melissa Lassig-Smith, Janine Stuart, Christopher Zappala, Rob Boots
{"title":"外源性褪黑素对危重患者谵妄和睡眠的影响:一项随机对照试验。","authors":"Judith Bellapart, Vinesh Appadurai, Melissa Lassig-Smith, Janine Stuart, Christopher Zappala, Rob Boots","doi":"10.1155/2020/3951828","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Sleep deprivation is a contributor for delirium in intensive care. Melatonin has been proposed as a pharmacological strategy to improve sleep, but studies have shown that the increase in plasma levels of melatonin do not correlate to a beneficial clinical effect; in addition, melatonin's short half-life may be a major limitation to achieving therapeutic levels. This study applies a previously published novel regimen of melatonin with proven sustained levels of melatonin during a 12 h period. In this study, the aim is to determine if such melatonin dosing positively influences on the sleep architecture and the incidence of delirium in intensive care.</p><p><strong>Methods: </strong>Single center, randomized control trial with consecutive recruitment over 5 years. Medical and surgical patients were in a recovery phase, all weaning from mechanical ventilation. Randomized allocation to placebo or enteral melatonin, using a previously described regimen (loading dose of 3 mg at 21 h, followed by 0.5 mg hourly maintenance dose until 03am through a nasogastric tube). Sleep recordings were performed using polysomnogram at baseline (prior to intervention) and the third night on melatonin (postintervention recording). Delirium was assessed using the Richmond Agitation and the Confusion Assessment Method Scales. Environmental light and noise levels were recorded using a luxmeter and sound meter.</p><p><strong>Results: </strong>80 patients were screened, but 33 were recruited. Sleep studies showed no statistical differences on arousal index or length of sleep. Baseline delirium scores showed no difference between groups when compared to postintervention scores. RASS scores were 1 in both groups at baseline, compared to zero (drug group) and 0.5 (placebo group) posttreatment. CAM scores were zero (drug group) and 1 (placebo group) at baseline, compared to zero (in both groups) postintervention.</p><p><strong>Conclusion: </strong>High levels of plasma melatonin during the overnight period of intensive care cohort patients did not improve sleep nor decreased the prevalence of delirium. This trial is registered with Anzctr.org.au/ACTRN12620000661976.aspx.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2020 ","pages":"3951828"},"PeriodicalIF":1.8000,"publicationDate":"2020-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/3951828","citationCount":"8","resultStr":"{\"title\":\"Effect of Exogenous Melatonin Administration in Critically Ill Patients on Delirium and Sleep: A Randomized Controlled Trial.\",\"authors\":\"Judith Bellapart, Vinesh Appadurai, Melissa Lassig-Smith, Janine Stuart, Christopher Zappala, Rob Boots\",\"doi\":\"10.1155/2020/3951828\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Sleep deprivation is a contributor for delirium in intensive care. Melatonin has been proposed as a pharmacological strategy to improve sleep, but studies have shown that the increase in plasma levels of melatonin do not correlate to a beneficial clinical effect; in addition, melatonin's short half-life may be a major limitation to achieving therapeutic levels. This study applies a previously published novel regimen of melatonin with proven sustained levels of melatonin during a 12 h period. In this study, the aim is to determine if such melatonin dosing positively influences on the sleep architecture and the incidence of delirium in intensive care.</p><p><strong>Methods: </strong>Single center, randomized control trial with consecutive recruitment over 5 years. Medical and surgical patients were in a recovery phase, all weaning from mechanical ventilation. Randomized allocation to placebo or enteral melatonin, using a previously described regimen (loading dose of 3 mg at 21 h, followed by 0.5 mg hourly maintenance dose until 03am through a nasogastric tube). Sleep recordings were performed using polysomnogram at baseline (prior to intervention) and the third night on melatonin (postintervention recording). Delirium was assessed using the Richmond Agitation and the Confusion Assessment Method Scales. Environmental light and noise levels were recorded using a luxmeter and sound meter.</p><p><strong>Results: </strong>80 patients were screened, but 33 were recruited. Sleep studies showed no statistical differences on arousal index or length of sleep. Baseline delirium scores showed no difference between groups when compared to postintervention scores. RASS scores were 1 in both groups at baseline, compared to zero (drug group) and 0.5 (placebo group) posttreatment. CAM scores were zero (drug group) and 1 (placebo group) at baseline, compared to zero (in both groups) postintervention.</p><p><strong>Conclusion: </strong>High levels of plasma melatonin during the overnight period of intensive care cohort patients did not improve sleep nor decreased the prevalence of delirium. This trial is registered with Anzctr.org.au/ACTRN12620000661976.aspx.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2020 \",\"pages\":\"3951828\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/3951828\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/3951828\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/3951828","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Effect of Exogenous Melatonin Administration in Critically Ill Patients on Delirium and Sleep: A Randomized Controlled Trial.
Introduction: Sleep deprivation is a contributor for delirium in intensive care. Melatonin has been proposed as a pharmacological strategy to improve sleep, but studies have shown that the increase in plasma levels of melatonin do not correlate to a beneficial clinical effect; in addition, melatonin's short half-life may be a major limitation to achieving therapeutic levels. This study applies a previously published novel regimen of melatonin with proven sustained levels of melatonin during a 12 h period. In this study, the aim is to determine if such melatonin dosing positively influences on the sleep architecture and the incidence of delirium in intensive care.
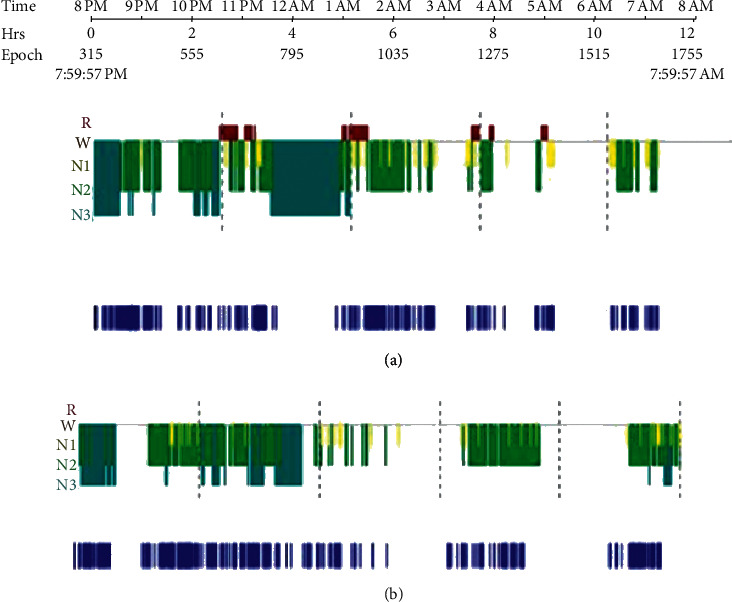
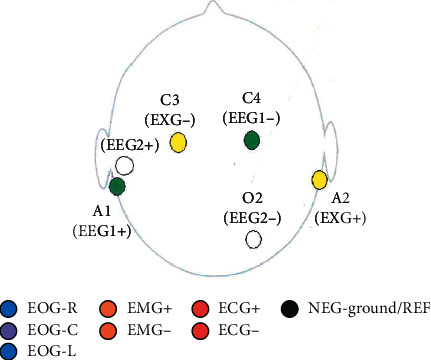
Methods: Single center, randomized control trial with consecutive recruitment over 5 years. Medical and surgical patients were in a recovery phase, all weaning from mechanical ventilation. Randomized allocation to placebo or enteral melatonin, using a previously described regimen (loading dose of 3 mg at 21 h, followed by 0.5 mg hourly maintenance dose until 03am through a nasogastric tube). Sleep recordings were performed using polysomnogram at baseline (prior to intervention) and the third night on melatonin (postintervention recording). Delirium was assessed using the Richmond Agitation and the Confusion Assessment Method Scales. Environmental light and noise levels were recorded using a luxmeter and sound meter.
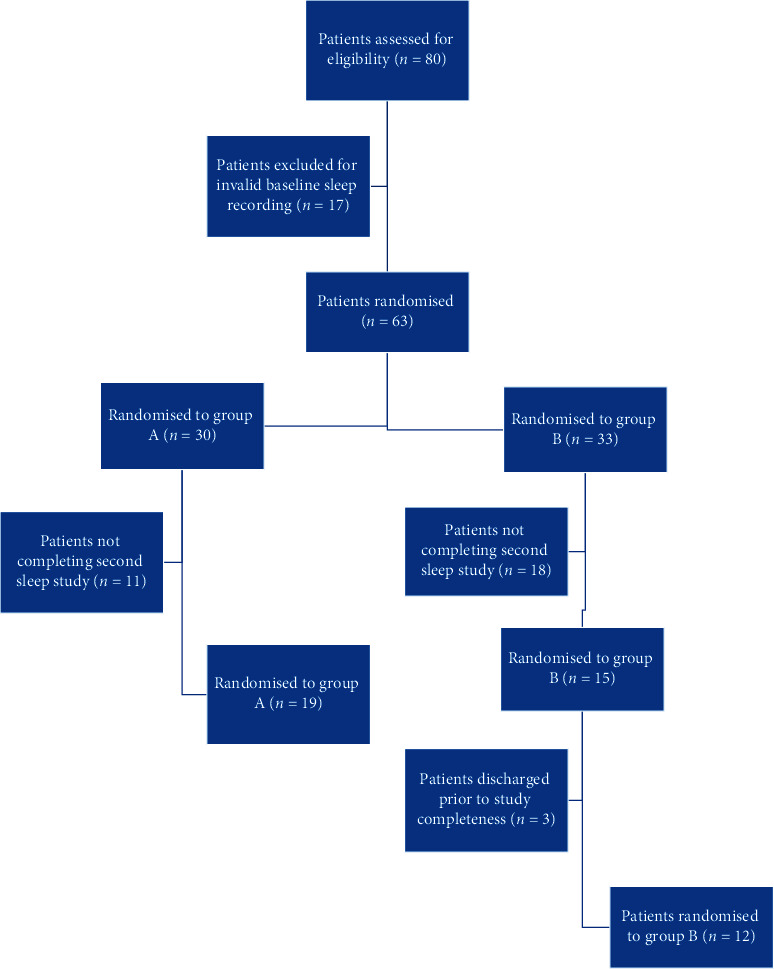
Results: 80 patients were screened, but 33 were recruited. Sleep studies showed no statistical differences on arousal index or length of sleep. Baseline delirium scores showed no difference between groups when compared to postintervention scores. RASS scores were 1 in both groups at baseline, compared to zero (drug group) and 0.5 (placebo group) posttreatment. CAM scores were zero (drug group) and 1 (placebo group) at baseline, compared to zero (in both groups) postintervention.
Conclusion: High levels of plasma melatonin during the overnight period of intensive care cohort patients did not improve sleep nor decreased the prevalence of delirium. This trial is registered with Anzctr.org.au/ACTRN12620000661976.aspx.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


