{"title":"社区获得性肺炎临床结果和护理措施过程的变化:系统回顾。","authors":"H Lawrence, W S Lim, T M McKeever","doi":"10.1186/s41479-020-00073-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Variation in outcomes of patients with community acquired pneumonia (CAP) has been reported in some, but not all, studies. Although some variation is expected, unwarranted variation in healthcare impacts patient outcomes and equity of care. The aim of this systematic review was to: i) summarise current evidence on regional and inter-hospital variation in the clinical outcomes and process of care measures of patients hospitalised with CAP and ii) assess the strength of this evidence.</p><p><strong>Methods: </strong>Databases were systematically searched from inception to February 2018 for relevant studies and data independently extracted by two investigators in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. Included studies enrolled adults hospitalised with CAP and reported a measure of variation between two or more units in healthcare outcomes or process of care measures. Outcomes of interest were mortality, length of hospital stay (LOS) and re-admission rates. A structured synthesis of the studies was performed.</p><p><strong>Results: </strong>Twenty-two studies were included in the analysis. The median number of units compared across studies was five (IQR 4-15). Evidence for variation in mortality between units was inconsistent; of eleven studies that performed statistical significance testing, five found significant variation. For LOS, of nine relevant studies, all found statistically significant variation. Four studies reported site of admission accounted for 1-24% of the total observed variation in LOS. A shorter LOS was not associated with increased mortality or readmission rates. For readmission, evidence was mixed; of seven studies, 4 found statistically significant variation. There was consistent evidence for variation in the use of intensive care, obtaining blood cultures on admission, receiving antibiotics within 8 h of admission and duration of intravenous antibiotics. Across all outcome measures, only one study accounted for natural variation between units in their analysis.</p><p><strong>Conclusion: </strong>There is consistent evidence of moderate quality for significant variation in length of stay and process of care measures but not for in-patient mortality or hospital re-admission. Evidence linking variation in outcomes with variation in process of care measures was limited; where present no difference in mortality was detected despite POC variation. Adjustment for natural variation within studies was lacking; the proportion of observed variation due to chance is not quantified by existing evidence.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":" ","pages":"10"},"PeriodicalIF":6.2000,"publicationDate":"2020-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s41479-020-00073-4","citationCount":"3","resultStr":"{\"title\":\"Variation in clinical outcomes and process of care measures in community acquired pneumonia: a systematic review.\",\"authors\":\"H Lawrence, W S Lim, T M McKeever\",\"doi\":\"10.1186/s41479-020-00073-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Variation in outcomes of patients with community acquired pneumonia (CAP) has been reported in some, but not all, studies. Although some variation is expected, unwarranted variation in healthcare impacts patient outcomes and equity of care. The aim of this systematic review was to: i) summarise current evidence on regional and inter-hospital variation in the clinical outcomes and process of care measures of patients hospitalised with CAP and ii) assess the strength of this evidence.</p><p><strong>Methods: </strong>Databases were systematically searched from inception to February 2018 for relevant studies and data independently extracted by two investigators in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. Included studies enrolled adults hospitalised with CAP and reported a measure of variation between two or more units in healthcare outcomes or process of care measures. Outcomes of interest were mortality, length of hospital stay (LOS) and re-admission rates. A structured synthesis of the studies was performed.</p><p><strong>Results: </strong>Twenty-two studies were included in the analysis. The median number of units compared across studies was five (IQR 4-15). Evidence for variation in mortality between units was inconsistent; of eleven studies that performed statistical significance testing, five found significant variation. For LOS, of nine relevant studies, all found statistically significant variation. Four studies reported site of admission accounted for 1-24% of the total observed variation in LOS. A shorter LOS was not associated with increased mortality or readmission rates. For readmission, evidence was mixed; of seven studies, 4 found statistically significant variation. There was consistent evidence for variation in the use of intensive care, obtaining blood cultures on admission, receiving antibiotics within 8 h of admission and duration of intravenous antibiotics. Across all outcome measures, only one study accounted for natural variation between units in their analysis.</p><p><strong>Conclusion: </strong>There is consistent evidence of moderate quality for significant variation in length of stay and process of care measures but not for in-patient mortality or hospital re-admission. Evidence linking variation in outcomes with variation in process of care measures was limited; where present no difference in mortality was detected despite POC variation. Adjustment for natural variation within studies was lacking; the proportion of observed variation due to chance is not quantified by existing evidence.</p>\",\"PeriodicalId\":45120,\"journal\":{\"name\":\"Pneumonia\",\"volume\":\" \",\"pages\":\"10\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2020-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s41479-020-00073-4\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pneumonia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41479-020-00073-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-020-00073-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Variation in clinical outcomes and process of care measures in community acquired pneumonia: a systematic review.
Background: Variation in outcomes of patients with community acquired pneumonia (CAP) has been reported in some, but not all, studies. Although some variation is expected, unwarranted variation in healthcare impacts patient outcomes and equity of care. The aim of this systematic review was to: i) summarise current evidence on regional and inter-hospital variation in the clinical outcomes and process of care measures of patients hospitalised with CAP and ii) assess the strength of this evidence.
Methods: Databases were systematically searched from inception to February 2018 for relevant studies and data independently extracted by two investigators in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. Included studies enrolled adults hospitalised with CAP and reported a measure of variation between two or more units in healthcare outcomes or process of care measures. Outcomes of interest were mortality, length of hospital stay (LOS) and re-admission rates. A structured synthesis of the studies was performed.
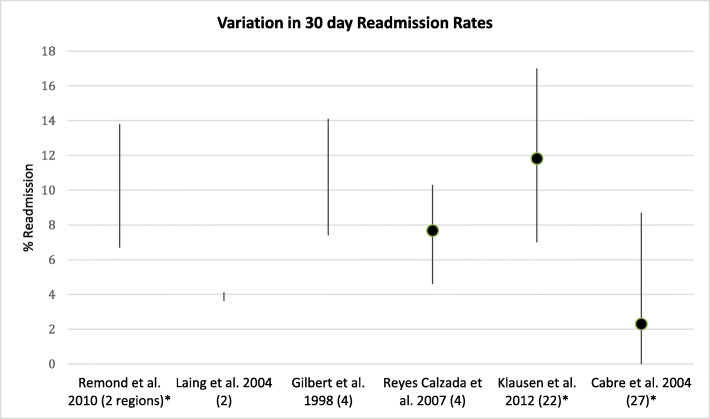
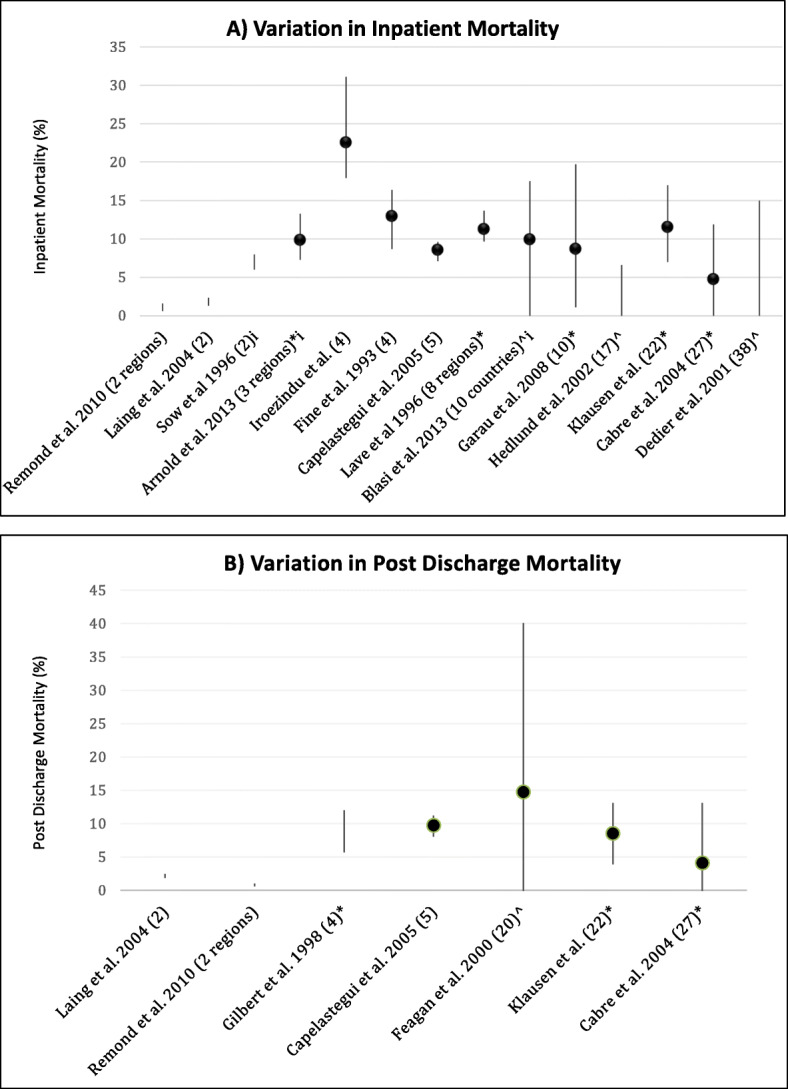
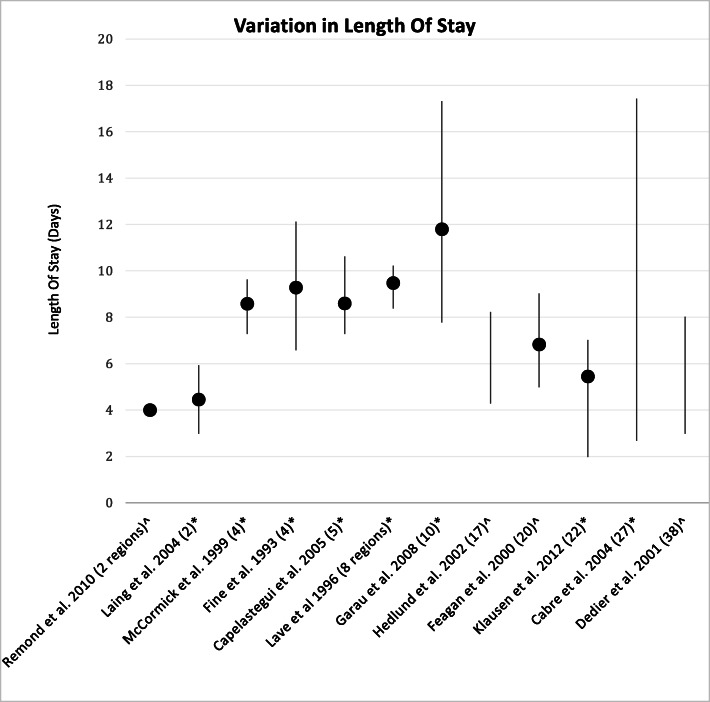
Results: Twenty-two studies were included in the analysis. The median number of units compared across studies was five (IQR 4-15). Evidence for variation in mortality between units was inconsistent; of eleven studies that performed statistical significance testing, five found significant variation. For LOS, of nine relevant studies, all found statistically significant variation. Four studies reported site of admission accounted for 1-24% of the total observed variation in LOS. A shorter LOS was not associated with increased mortality or readmission rates. For readmission, evidence was mixed; of seven studies, 4 found statistically significant variation. There was consistent evidence for variation in the use of intensive care, obtaining blood cultures on admission, receiving antibiotics within 8 h of admission and duration of intravenous antibiotics. Across all outcome measures, only one study accounted for natural variation between units in their analysis.
Conclusion: There is consistent evidence of moderate quality for significant variation in length of stay and process of care measures but not for in-patient mortality or hospital re-admission. Evidence linking variation in outcomes with variation in process of care measures was limited; where present no difference in mortality was detected despite POC variation. Adjustment for natural variation within studies was lacking; the proportion of observed variation due to chance is not quantified by existing evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


