Antti Valtola, James D Morse, Pawel Florkiewicz, Heidi Hautajärvi, Pasi Lahtinen, Tadeusz Musialowicz, Brian J Anderson, Veli-Pekka Ranta, Hannu Kokki
{"title":"冠状动脉搭桥术患者口服羟考酮的生物利用度-一项随机试验。","authors":"Antti Valtola, James D Morse, Pawel Florkiewicz, Heidi Hautajärvi, Pasi Lahtinen, Tadeusz Musialowicz, Brian J Anderson, Veli-Pekka Ranta, Hannu Kokki","doi":"10.1080/21556660.2020.1797753","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Pain after coronary artery by-pass (CAB) surgery is severe. Analgesic administration by mouth is unreliable until after gastrointestinal function has recovered. We evaluated the bioavailability of oxycodone co-administered with naloxone by mouth in patients after CAB surgery using either a conventional extracorporeal circulation (CECC) or off-pump surgery (OPCAB).</p><p><strong>Methods: </strong>Twenty-four patients, 50-73 years, 12 with CECC and 12 with OPCAB, were administered a 10/5 mg oxycodone-naloxone controlled-release tablet by mouth on the preoperative day and for the first seven postoperative days (PODs) thereafter. Blood samples were collected up to 24 h after the preoperative administration, and then randomly either on POD1 and POD3 or on POD2 and POD4. The oxycodone concentration in plasma was analyzed using liquid chromatography-mass spectrometry.</p><p><strong>Results: </strong>On POD1 oxycodone absorption was markedly delayed in five of six patients after CECC and in all six patients after OPCAB surgery; median of t<sub>max</sub> after CECC 630 [range 270-1420] minutes and after OPCAB 1020 [720-1410] minutes, compared to median of 120-315 min preoperatively and on POD2-POD4. The carry-over corrected AUC<sub>0-24</sub> values on the PODs did not differ from the preoperative values, but were higher on POD3 compared with POD1 in both CECC and OPCAB groups. The rate and extent of oxycodone absorption equaled preoperative values on POD2 and onwards in patients with CAB surgery.</p><p><strong>Conclusions: </strong>Bioavailability of oxycodone by mouth was similar after CAB surgery <i>via</i> CECC or having OPCAB. Data indicate that POD2 is an appropriate time to start oxycodone administration by mouth after CAB surgery.</p>","PeriodicalId":15631,"journal":{"name":"Journal of Drug Assessment","volume":"9 1","pages":"117-128"},"PeriodicalIF":2.4000,"publicationDate":"2020-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/21556660.2020.1797753","citationCount":"3","resultStr":"{\"title\":\"Bioavailability of oxycodone by mouth in coronary artery bypass surgery patients - a randomized trial.\",\"authors\":\"Antti Valtola, James D Morse, Pawel Florkiewicz, Heidi Hautajärvi, Pasi Lahtinen, Tadeusz Musialowicz, Brian J Anderson, Veli-Pekka Ranta, Hannu Kokki\",\"doi\":\"10.1080/21556660.2020.1797753\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Pain after coronary artery by-pass (CAB) surgery is severe. Analgesic administration by mouth is unreliable until after gastrointestinal function has recovered. We evaluated the bioavailability of oxycodone co-administered with naloxone by mouth in patients after CAB surgery using either a conventional extracorporeal circulation (CECC) or off-pump surgery (OPCAB).</p><p><strong>Methods: </strong>Twenty-four patients, 50-73 years, 12 with CECC and 12 with OPCAB, were administered a 10/5 mg oxycodone-naloxone controlled-release tablet by mouth on the preoperative day and for the first seven postoperative days (PODs) thereafter. Blood samples were collected up to 24 h after the preoperative administration, and then randomly either on POD1 and POD3 or on POD2 and POD4. The oxycodone concentration in plasma was analyzed using liquid chromatography-mass spectrometry.</p><p><strong>Results: </strong>On POD1 oxycodone absorption was markedly delayed in five of six patients after CECC and in all six patients after OPCAB surgery; median of t<sub>max</sub> after CECC 630 [range 270-1420] minutes and after OPCAB 1020 [720-1410] minutes, compared to median of 120-315 min preoperatively and on POD2-POD4. The carry-over corrected AUC<sub>0-24</sub> values on the PODs did not differ from the preoperative values, but were higher on POD3 compared with POD1 in both CECC and OPCAB groups. The rate and extent of oxycodone absorption equaled preoperative values on POD2 and onwards in patients with CAB surgery.</p><p><strong>Conclusions: </strong>Bioavailability of oxycodone by mouth was similar after CAB surgery <i>via</i> CECC or having OPCAB. Data indicate that POD2 is an appropriate time to start oxycodone administration by mouth after CAB surgery.</p>\",\"PeriodicalId\":15631,\"journal\":{\"name\":\"Journal of Drug Assessment\",\"volume\":\"9 1\",\"pages\":\"117-128\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2020-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1080/21556660.2020.1797753\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Drug Assessment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/21556660.2020.1797753\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Drug Assessment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/21556660.2020.1797753","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Bioavailability of oxycodone by mouth in coronary artery bypass surgery patients - a randomized trial.
Objective: Pain after coronary artery by-pass (CAB) surgery is severe. Analgesic administration by mouth is unreliable until after gastrointestinal function has recovered. We evaluated the bioavailability of oxycodone co-administered with naloxone by mouth in patients after CAB surgery using either a conventional extracorporeal circulation (CECC) or off-pump surgery (OPCAB).
Methods: Twenty-four patients, 50-73 years, 12 with CECC and 12 with OPCAB, were administered a 10/5 mg oxycodone-naloxone controlled-release tablet by mouth on the preoperative day and for the first seven postoperative days (PODs) thereafter. Blood samples were collected up to 24 h after the preoperative administration, and then randomly either on POD1 and POD3 or on POD2 and POD4. The oxycodone concentration in plasma was analyzed using liquid chromatography-mass spectrometry.
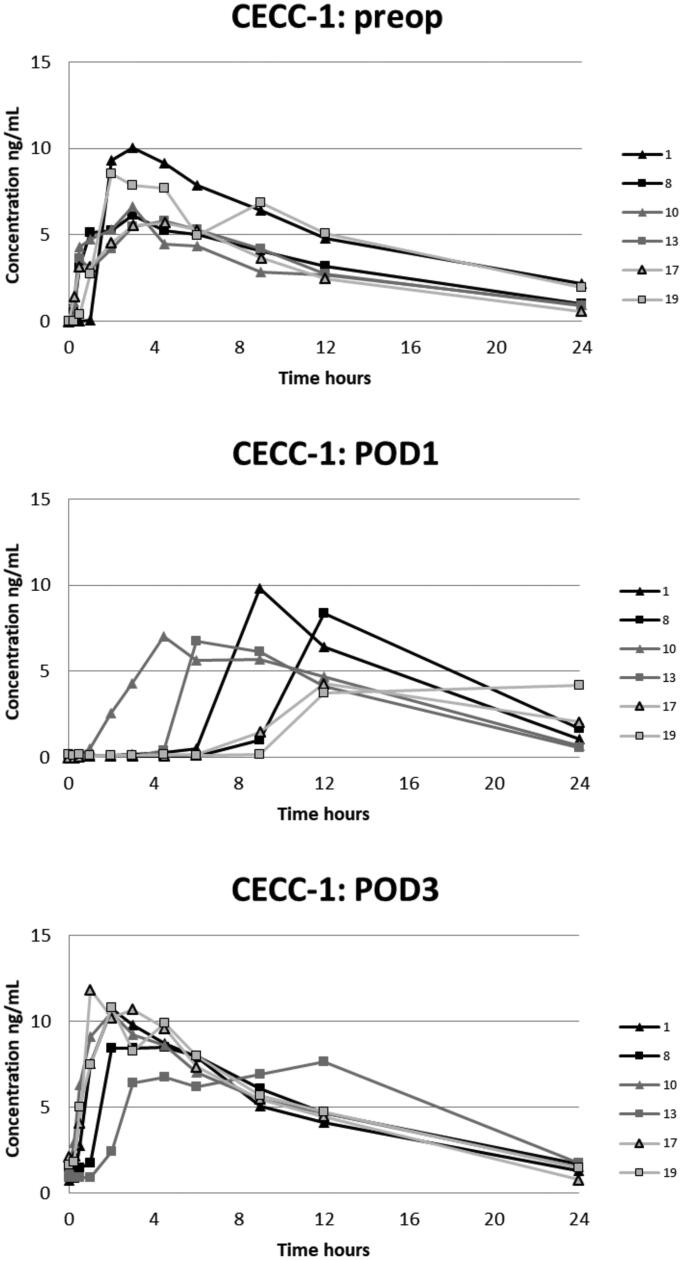
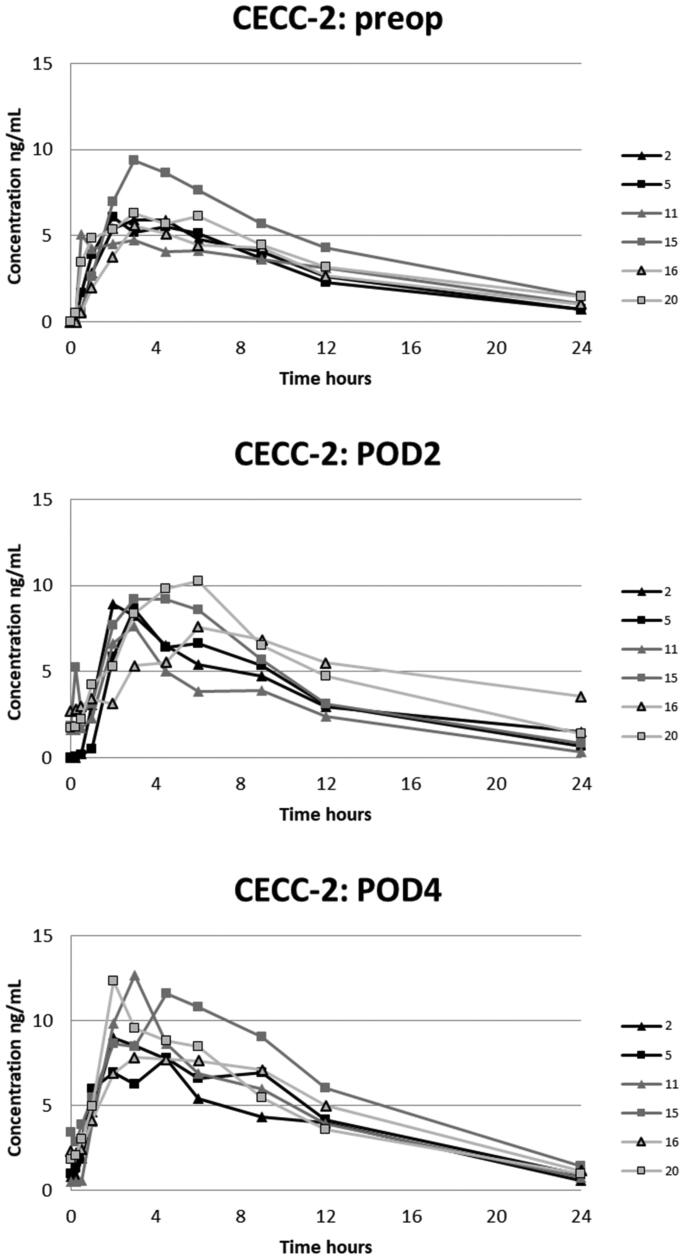
Results: On POD1 oxycodone absorption was markedly delayed in five of six patients after CECC and in all six patients after OPCAB surgery; median of tmax after CECC 630 [range 270-1420] minutes and after OPCAB 1020 [720-1410] minutes, compared to median of 120-315 min preoperatively and on POD2-POD4. The carry-over corrected AUC0-24 values on the PODs did not differ from the preoperative values, but were higher on POD3 compared with POD1 in both CECC and OPCAB groups. The rate and extent of oxycodone absorption equaled preoperative values on POD2 and onwards in patients with CAB surgery.
Conclusions: Bioavailability of oxycodone by mouth was similar after CAB surgery via CECC or having OPCAB. Data indicate that POD2 is an appropriate time to start oxycodone administration by mouth after CAB surgery.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


