{"title":"腰椎间盘退变与腰骶神经病变的临床表现。","authors":"Worku Abie Liyew","doi":"10.1155/2020/2919625","DOIUrl":null,"url":null,"abstract":"<p><p>Lumbar disc degeneration is defined as the wear and tear of lumbar intervertebral disc, and it is mainly occurring at L3-L4 and L4-S1 vertebrae. Lumbar disc degeneration may lead to disc bulging, osteophytes, loss of disc space, and compression and irritation of the adjacent nerve root. Clinical presentations associated with lumbar disc degeneration and lumbosacral nerve lesion are discogenic pain, radical pain, muscular weakness, and cutaneous. Discogenic pain is usually felt in the lumbar region, or sometimes, it may feel in the buttocks, down to the upper thighs, and it is typically presented with sudden forced flexion and/or rotational moment. Radical pain, muscular weakness, and sensory defects associated with lumbosacral nerve lesions are distributed on lower extremities, the buttock, lower abdomen, and groin region. A lumbosacral plexus lesion presents different symptoms in the territories of the lumbar and sacral nerves. Patients with lumbar plexus lesion clinically present with weakness of hip flexion, knee extension, thigh adduction, and sensory loss in the lower abdomen, inguinal region, and over the entire medial, lateral, and anterior surfaces of the thigh and the medial lower leg, while sacral plexus lesion presents clinical symptoms at nerve fibers destined for the sciatic nerve, common peroneal nerve, and pudendal nerve. Weakness of ankle inversion, plantar flexion, and foot drop are the main clinical manifestations of the sacral plexus lesion area. Numbness and decreased sensation are also present along the anterolateral calf and dorsum of the foot. On examination, foot eversion is usually stronger than foot dorsiflexion. The patients may also present with pain and difficulty of bowel movements, sexual dysfunction assessments, and loss of cutaneous sensation in the areas of the anal canal, anus, labia major, labia minor, clitoris, penis, and scrotum.</p>","PeriodicalId":51715,"journal":{"name":"International Journal of Rheumatology","volume":"2020 ","pages":"2919625"},"PeriodicalIF":2.3000,"publicationDate":"2020-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/2919625","citationCount":"11","resultStr":"{\"title\":\"Clinical Presentations of Lumbar Disc Degeneration and Lumbosacral Nerve Lesions.\",\"authors\":\"Worku Abie Liyew\",\"doi\":\"10.1155/2020/2919625\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Lumbar disc degeneration is defined as the wear and tear of lumbar intervertebral disc, and it is mainly occurring at L3-L4 and L4-S1 vertebrae. Lumbar disc degeneration may lead to disc bulging, osteophytes, loss of disc space, and compression and irritation of the adjacent nerve root. Clinical presentations associated with lumbar disc degeneration and lumbosacral nerve lesion are discogenic pain, radical pain, muscular weakness, and cutaneous. Discogenic pain is usually felt in the lumbar region, or sometimes, it may feel in the buttocks, down to the upper thighs, and it is typically presented with sudden forced flexion and/or rotational moment. Radical pain, muscular weakness, and sensory defects associated with lumbosacral nerve lesions are distributed on lower extremities, the buttock, lower abdomen, and groin region. A lumbosacral plexus lesion presents different symptoms in the territories of the lumbar and sacral nerves. Patients with lumbar plexus lesion clinically present with weakness of hip flexion, knee extension, thigh adduction, and sensory loss in the lower abdomen, inguinal region, and over the entire medial, lateral, and anterior surfaces of the thigh and the medial lower leg, while sacral plexus lesion presents clinical symptoms at nerve fibers destined for the sciatic nerve, common peroneal nerve, and pudendal nerve. Weakness of ankle inversion, plantar flexion, and foot drop are the main clinical manifestations of the sacral plexus lesion area. Numbness and decreased sensation are also present along the anterolateral calf and dorsum of the foot. On examination, foot eversion is usually stronger than foot dorsiflexion. The patients may also present with pain and difficulty of bowel movements, sexual dysfunction assessments, and loss of cutaneous sensation in the areas of the anal canal, anus, labia major, labia minor, clitoris, penis, and scrotum.</p>\",\"PeriodicalId\":51715,\"journal\":{\"name\":\"International Journal of Rheumatology\",\"volume\":\"2020 \",\"pages\":\"2919625\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2020-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/2919625\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/2919625\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/2919625","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Clinical Presentations of Lumbar Disc Degeneration and Lumbosacral Nerve Lesions.
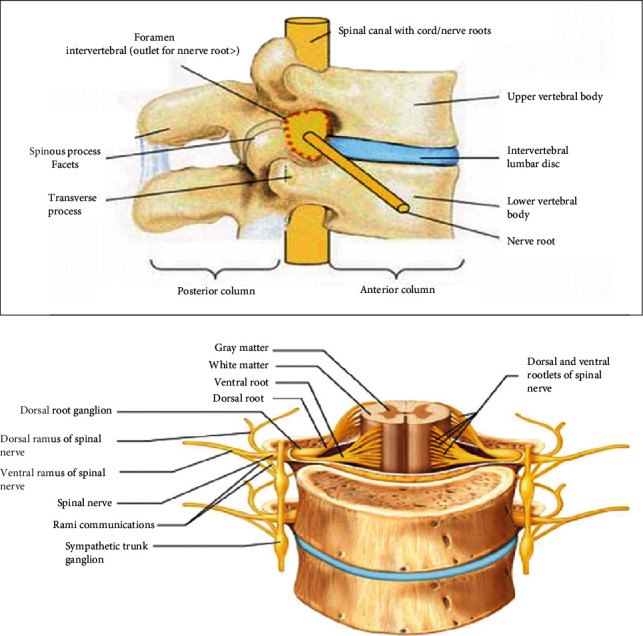
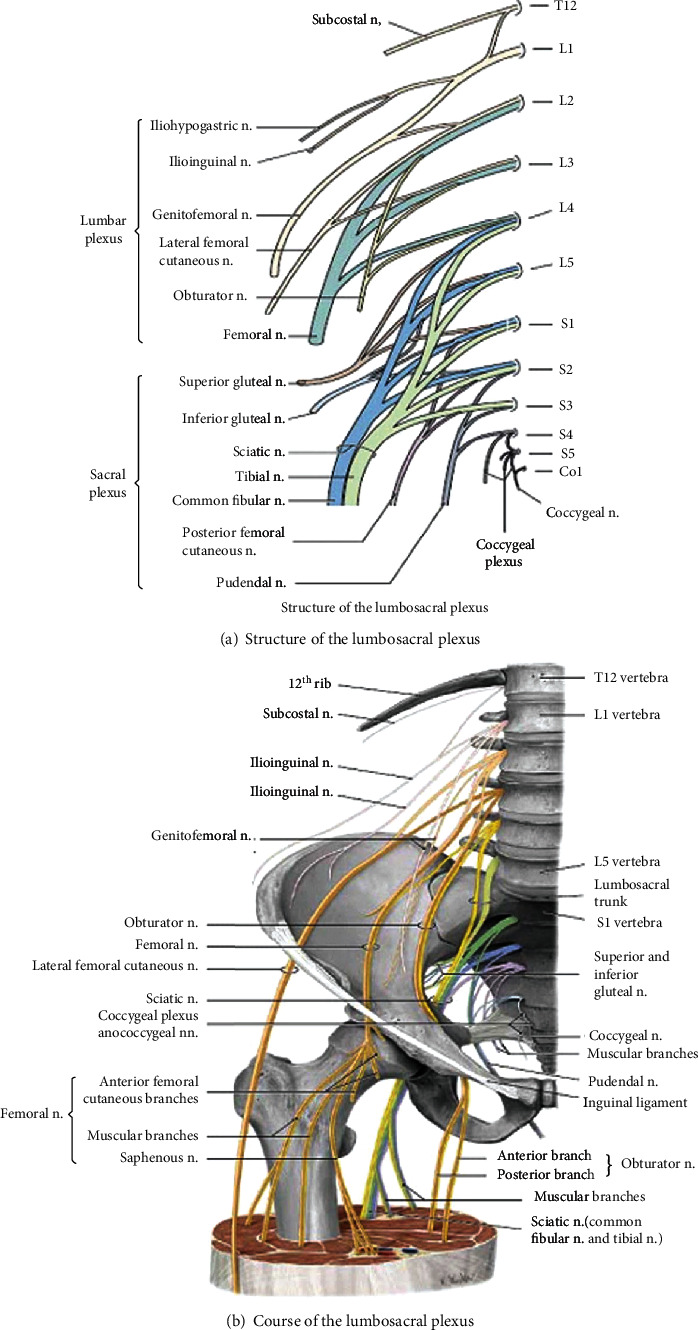
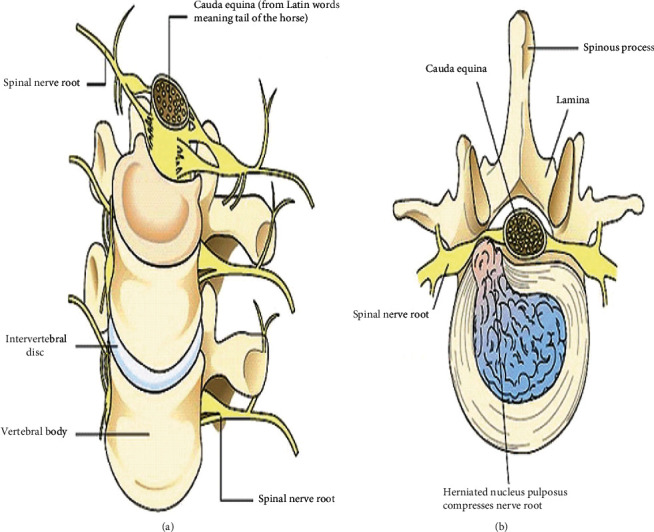
Lumbar disc degeneration is defined as the wear and tear of lumbar intervertebral disc, and it is mainly occurring at L3-L4 and L4-S1 vertebrae. Lumbar disc degeneration may lead to disc bulging, osteophytes, loss of disc space, and compression and irritation of the adjacent nerve root. Clinical presentations associated with lumbar disc degeneration and lumbosacral nerve lesion are discogenic pain, radical pain, muscular weakness, and cutaneous. Discogenic pain is usually felt in the lumbar region, or sometimes, it may feel in the buttocks, down to the upper thighs, and it is typically presented with sudden forced flexion and/or rotational moment. Radical pain, muscular weakness, and sensory defects associated with lumbosacral nerve lesions are distributed on lower extremities, the buttock, lower abdomen, and groin region. A lumbosacral plexus lesion presents different symptoms in the territories of the lumbar and sacral nerves. Patients with lumbar plexus lesion clinically present with weakness of hip flexion, knee extension, thigh adduction, and sensory loss in the lower abdomen, inguinal region, and over the entire medial, lateral, and anterior surfaces of the thigh and the medial lower leg, while sacral plexus lesion presents clinical symptoms at nerve fibers destined for the sciatic nerve, common peroneal nerve, and pudendal nerve. Weakness of ankle inversion, plantar flexion, and foot drop are the main clinical manifestations of the sacral plexus lesion area. Numbness and decreased sensation are also present along the anterolateral calf and dorsum of the foot. On examination, foot eversion is usually stronger than foot dorsiflexion. The patients may also present with pain and difficulty of bowel movements, sexual dysfunction assessments, and loss of cutaneous sensation in the areas of the anal canal, anus, labia major, labia minor, clitoris, penis, and scrotum.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


