Rawlance Ndejjo, Rhoda K Wanyenze, Fred Nuwaha, Hilde Bastiaens, Geofrey Musinguzi
{"title":"利用实施研究综合框架在乌干达穆科诺和布伊奎地区实施社区心血管疾病预防方案的障碍和促进因素。","authors":"Rawlance Ndejjo, Rhoda K Wanyenze, Fred Nuwaha, Hilde Bastiaens, Geofrey Musinguzi","doi":"10.1186/s13012-020-01065-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In low- and middle-income countries, there is an increasing attention towards community approaches to deal with the growing burden of cardiovascular disease (CVD). However, few studies have explored the implementation processes of such interventions to inform their scale up and sustainability. Using the consolidated framework for implementation research (CFIR), we examined the barriers and facilitators influencing the implementation of a community CVD programme led by community health workers (CHWs) in Mukono and Buikwe districts in Uganda.</p><p><strong>Methods: </strong>This qualitative study is a process evaluation of an ongoing type II hybrid stepped wedge cluster trial guided by the CFIR. Data for this analysis were collected through regular meetings and focus group discussions (FGDs) conducted during the first cycle (6 months) of intervention implementation. A total of 20 CHWs participated in the implementation programme in 20 villages during the first cycle. Meeting reports and FGD transcripts were analysed following inductive thematic analysis with the aid of Nvivo 12.6 to generate emerging themes and sub-themes and thereafter deductive analysis was used to map themes and sub-themes onto the CFIR domains and constructs.</p><p><strong>Results: </strong>The barriers to intervention implementation were the complexity of the intervention (complexity), compatibility with community culture (culture), the lack of an enabling environment for behaviour change (patient needs and resources) and mistrust of CHWs by community members (relative priority). In addition, the low community awareness of CVD (tension for change), competing demands (other personal attributes) and unfavourable policies (external policy and incentives) impeded intervention implementation. On the other hand, facilitators of intervention implementation were availability of inputs and protective equipment (design quality and packaging), training of CHWs (Available resources), working with community structures including leaders and groups (process-opinion leaders), frequent support supervision and engagements (process-formally appointed internal implementation leaders) and access to quality health services (process-champions).</p><p><strong>Conclusion: </strong>Using the CFIR, we identified drivers of implementation success or failure for a community CVD prevention programme in a low-income context. These findings are key to inform the design of impactful, scalable and sustainable CHW programmes for non-communicable diseases prevention and control.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"106"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13012-020-01065-0","citationCount":"12","resultStr":"{\"title\":\"Barriers and facilitators of implementation of a community cardiovascular disease prevention programme in Mukono and Buikwe districts in Uganda using the Consolidated Framework for Implementation Research.\",\"authors\":\"Rawlance Ndejjo, Rhoda K Wanyenze, Fred Nuwaha, Hilde Bastiaens, Geofrey Musinguzi\",\"doi\":\"10.1186/s13012-020-01065-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In low- and middle-income countries, there is an increasing attention towards community approaches to deal with the growing burden of cardiovascular disease (CVD). However, few studies have explored the implementation processes of such interventions to inform their scale up and sustainability. Using the consolidated framework for implementation research (CFIR), we examined the barriers and facilitators influencing the implementation of a community CVD programme led by community health workers (CHWs) in Mukono and Buikwe districts in Uganda.</p><p><strong>Methods: </strong>This qualitative study is a process evaluation of an ongoing type II hybrid stepped wedge cluster trial guided by the CFIR. Data for this analysis were collected through regular meetings and focus group discussions (FGDs) conducted during the first cycle (6 months) of intervention implementation. A total of 20 CHWs participated in the implementation programme in 20 villages during the first cycle. Meeting reports and FGD transcripts were analysed following inductive thematic analysis with the aid of Nvivo 12.6 to generate emerging themes and sub-themes and thereafter deductive analysis was used to map themes and sub-themes onto the CFIR domains and constructs.</p><p><strong>Results: </strong>The barriers to intervention implementation were the complexity of the intervention (complexity), compatibility with community culture (culture), the lack of an enabling environment for behaviour change (patient needs and resources) and mistrust of CHWs by community members (relative priority). In addition, the low community awareness of CVD (tension for change), competing demands (other personal attributes) and unfavourable policies (external policy and incentives) impeded intervention implementation. On the other hand, facilitators of intervention implementation were availability of inputs and protective equipment (design quality and packaging), training of CHWs (Available resources), working with community structures including leaders and groups (process-opinion leaders), frequent support supervision and engagements (process-formally appointed internal implementation leaders) and access to quality health services (process-champions).</p><p><strong>Conclusion: </strong>Using the CFIR, we identified drivers of implementation success or failure for a community CVD prevention programme in a low-income context. These findings are key to inform the design of impactful, scalable and sustainable CHW programmes for non-communicable diseases prevention and control.</p>\",\"PeriodicalId\":417097,\"journal\":{\"name\":\"Implementation Science : IS\",\"volume\":\" \",\"pages\":\"106\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-12-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13012-020-01065-0\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation Science : IS\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13012-020-01065-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13012-020-01065-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Barriers and facilitators of implementation of a community cardiovascular disease prevention programme in Mukono and Buikwe districts in Uganda using the Consolidated Framework for Implementation Research.
Background: In low- and middle-income countries, there is an increasing attention towards community approaches to deal with the growing burden of cardiovascular disease (CVD). However, few studies have explored the implementation processes of such interventions to inform their scale up and sustainability. Using the consolidated framework for implementation research (CFIR), we examined the barriers and facilitators influencing the implementation of a community CVD programme led by community health workers (CHWs) in Mukono and Buikwe districts in Uganda.
Methods: This qualitative study is a process evaluation of an ongoing type II hybrid stepped wedge cluster trial guided by the CFIR. Data for this analysis were collected through regular meetings and focus group discussions (FGDs) conducted during the first cycle (6 months) of intervention implementation. A total of 20 CHWs participated in the implementation programme in 20 villages during the first cycle. Meeting reports and FGD transcripts were analysed following inductive thematic analysis with the aid of Nvivo 12.6 to generate emerging themes and sub-themes and thereafter deductive analysis was used to map themes and sub-themes onto the CFIR domains and constructs.
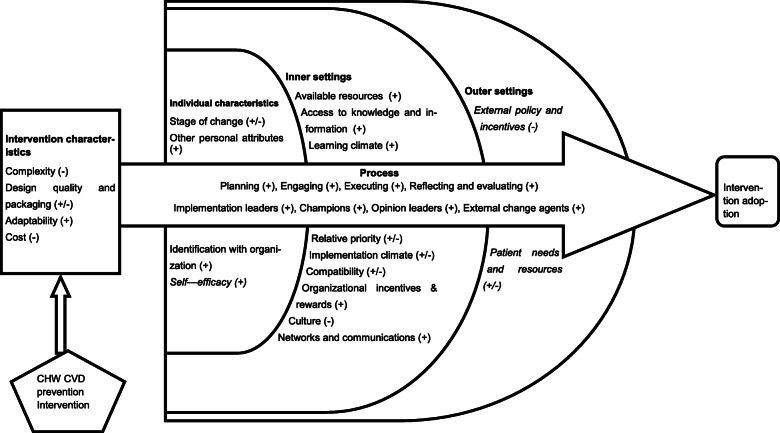
Results: The barriers to intervention implementation were the complexity of the intervention (complexity), compatibility with community culture (culture), the lack of an enabling environment for behaviour change (patient needs and resources) and mistrust of CHWs by community members (relative priority). In addition, the low community awareness of CVD (tension for change), competing demands (other personal attributes) and unfavourable policies (external policy and incentives) impeded intervention implementation. On the other hand, facilitators of intervention implementation were availability of inputs and protective equipment (design quality and packaging), training of CHWs (Available resources), working with community structures including leaders and groups (process-opinion leaders), frequent support supervision and engagements (process-formally appointed internal implementation leaders) and access to quality health services (process-champions).
Conclusion: Using the CFIR, we identified drivers of implementation success or failure for a community CVD prevention programme in a low-income context. These findings are key to inform the design of impactful, scalable and sustainable CHW programmes for non-communicable diseases prevention and control.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


