Edward Griffin, Chris Hyde, Linda Long, Jo Varley-Campbell, Helen Coelho, Sophie Robinson, Tristan Snowsill
{"title":"肺癌筛查低剂量计算机断层扫描:在英国使用新开发的基于自然历史的经济模型的替代方案的成本效益分析。","authors":"Edward Griffin, Chris Hyde, Linda Long, Jo Varley-Campbell, Helen Coelho, Sophie Robinson, Tristan Snowsill","doi":"10.1186/s41512-020-00087-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A systematic review of economic evaluations for lung cancer identified no economic models of the UK setting based on disease natural history. We first sought to develop a new model of natural history for population screening, then sought to explore the cost-effectiveness of multiple alternative potential programmes.</p><p><strong>Methods: </strong>An individual patient model (ENaBL) was constructed in MS Excel® and calibrated against data from the US National Lung Screening Trial. Costs were taken from the UK Lung Cancer Screening Trial and took the perspective of the NHS and PSS. Simulants were current or former smokers aged between 55 and 80 years and so at a higher risk of lung cancer relative to the general population. Subgroups were defined by further restricting age and risk of lung cancer as predicted by patient self-questionnaire. Programme designs were single, triple, annual and biennial arrangements of LDCT screens, thereby examining number and interval length. Forty-eight distinct screening strategies were compared to the current practice of no screening. The primary outcome was incremental cost-effectiveness of strategies (additional cost per QALY gained).</p><p><strong>Results: </strong>LDCT screening is predicted to bring forward the stage distribution at diagnosis and reduce lung cancer mortality, with decreases versus no screening ranging from 4.2 to 7.7% depending on screen frequency. Overall healthcare costs are predicted to increase; treatment cost savings from earlier detection are outweighed by the costs of over-diagnosis. Single-screen programmes for people 55-75 or 60-75 years with ≥ 3% predicted lung cancer risk may be cost-effective at the £30,000 per QALY threshold (respective ICERs of £28,784 and £28,169 per QALY gained). Annual and biennial screening programmes were not predicted to be cost-effective at any cost-effectiveness threshold.</p><p><strong>Limitations: </strong>LDCT performance was unaffected by lung cancer type, stage or location and the impact of a national screening programme of smoking behaviour was not included.</p><p><strong>Conclusion: </strong>Lung cancer screening may not be cost-effective at the threshold of £20,000 per QALY commonly used in the UK but may be cost-effective at the higher threshold of £30,000 per QALY.</p>","PeriodicalId":72800,"journal":{"name":"Diagnostic and prognostic research","volume":"4 1","pages":"20"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s41512-020-00087-y","citationCount":"14","resultStr":"{\"title\":\"Lung cancer screening by low-dose computed tomography: a cost-effectiveness analysis of alternative programmes in the UK using a newly developed natural history-based economic model.\",\"authors\":\"Edward Griffin, Chris Hyde, Linda Long, Jo Varley-Campbell, Helen Coelho, Sophie Robinson, Tristan Snowsill\",\"doi\":\"10.1186/s41512-020-00087-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A systematic review of economic evaluations for lung cancer identified no economic models of the UK setting based on disease natural history. We first sought to develop a new model of natural history for population screening, then sought to explore the cost-effectiveness of multiple alternative potential programmes.</p><p><strong>Methods: </strong>An individual patient model (ENaBL) was constructed in MS Excel® and calibrated against data from the US National Lung Screening Trial. Costs were taken from the UK Lung Cancer Screening Trial and took the perspective of the NHS and PSS. Simulants were current or former smokers aged between 55 and 80 years and so at a higher risk of lung cancer relative to the general population. Subgroups were defined by further restricting age and risk of lung cancer as predicted by patient self-questionnaire. Programme designs were single, triple, annual and biennial arrangements of LDCT screens, thereby examining number and interval length. Forty-eight distinct screening strategies were compared to the current practice of no screening. The primary outcome was incremental cost-effectiveness of strategies (additional cost per QALY gained).</p><p><strong>Results: </strong>LDCT screening is predicted to bring forward the stage distribution at diagnosis and reduce lung cancer mortality, with decreases versus no screening ranging from 4.2 to 7.7% depending on screen frequency. Overall healthcare costs are predicted to increase; treatment cost savings from earlier detection are outweighed by the costs of over-diagnosis. Single-screen programmes for people 55-75 or 60-75 years with ≥ 3% predicted lung cancer risk may be cost-effective at the £30,000 per QALY threshold (respective ICERs of £28,784 and £28,169 per QALY gained). Annual and biennial screening programmes were not predicted to be cost-effective at any cost-effectiveness threshold.</p><p><strong>Limitations: </strong>LDCT performance was unaffected by lung cancer type, stage or location and the impact of a national screening programme of smoking behaviour was not included.</p><p><strong>Conclusion: </strong>Lung cancer screening may not be cost-effective at the threshold of £20,000 per QALY commonly used in the UK but may be cost-effective at the higher threshold of £30,000 per QALY.</p>\",\"PeriodicalId\":72800,\"journal\":{\"name\":\"Diagnostic and prognostic research\",\"volume\":\"4 1\",\"pages\":\"20\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-12-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s41512-020-00087-y\",\"citationCount\":\"14\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diagnostic and prognostic research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41512-020-00087-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic and prognostic research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41512-020-00087-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Lung cancer screening by low-dose computed tomography: a cost-effectiveness analysis of alternative programmes in the UK using a newly developed natural history-based economic model.
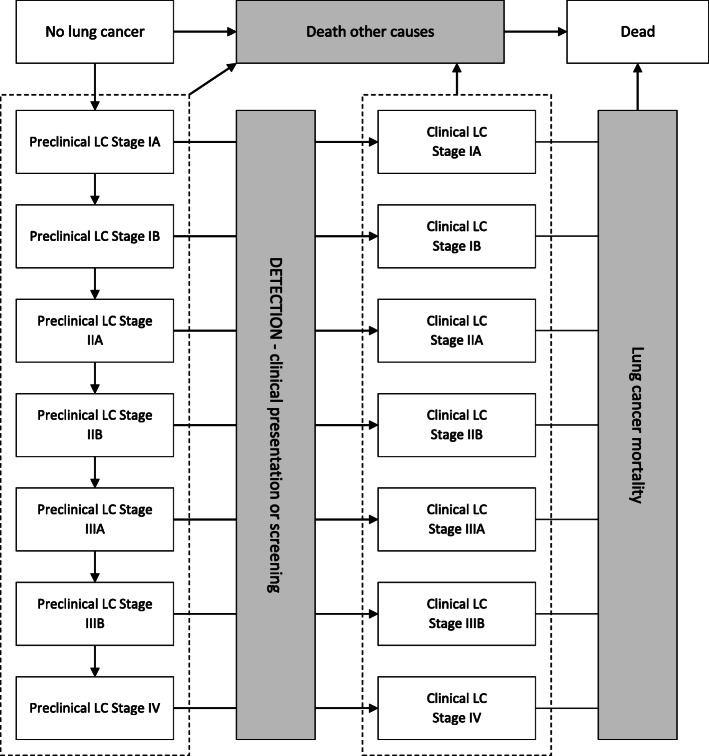
Background: A systematic review of economic evaluations for lung cancer identified no economic models of the UK setting based on disease natural history. We first sought to develop a new model of natural history for population screening, then sought to explore the cost-effectiveness of multiple alternative potential programmes.
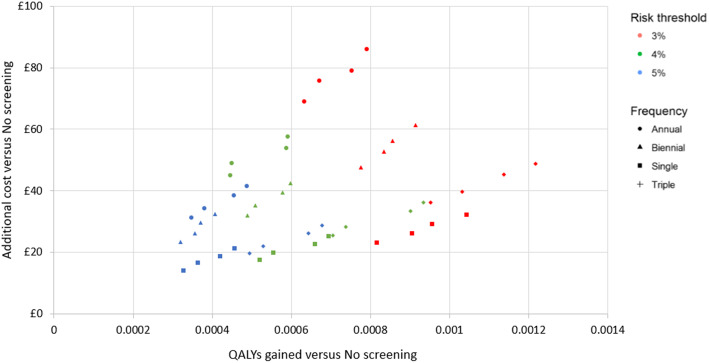
Methods: An individual patient model (ENaBL) was constructed in MS Excel® and calibrated against data from the US National Lung Screening Trial. Costs were taken from the UK Lung Cancer Screening Trial and took the perspective of the NHS and PSS. Simulants were current or former smokers aged between 55 and 80 years and so at a higher risk of lung cancer relative to the general population. Subgroups were defined by further restricting age and risk of lung cancer as predicted by patient self-questionnaire. Programme designs were single, triple, annual and biennial arrangements of LDCT screens, thereby examining number and interval length. Forty-eight distinct screening strategies were compared to the current practice of no screening. The primary outcome was incremental cost-effectiveness of strategies (additional cost per QALY gained).
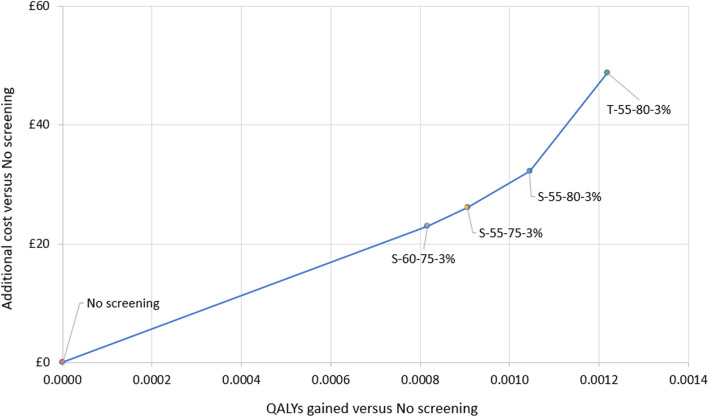
Results: LDCT screening is predicted to bring forward the stage distribution at diagnosis and reduce lung cancer mortality, with decreases versus no screening ranging from 4.2 to 7.7% depending on screen frequency. Overall healthcare costs are predicted to increase; treatment cost savings from earlier detection are outweighed by the costs of over-diagnosis. Single-screen programmes for people 55-75 or 60-75 years with ≥ 3% predicted lung cancer risk may be cost-effective at the £30,000 per QALY threshold (respective ICERs of £28,784 and £28,169 per QALY gained). Annual and biennial screening programmes were not predicted to be cost-effective at any cost-effectiveness threshold.
Limitations: LDCT performance was unaffected by lung cancer type, stage or location and the impact of a national screening programme of smoking behaviour was not included.
Conclusion: Lung cancer screening may not be cost-effective at the threshold of £20,000 per QALY commonly used in the UK but may be cost-effective at the higher threshold of £30,000 per QALY.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


